

Petrous apex cephaloceles
- PMID: 11733318
- PMCID: PMC7973833
Petrous apex cephaloceles
Abstract
Background and purpose: Petrous apex cephaloceles (PACs) are uncommon lesions that are usually incidental but may be symptomatic. We reviewed MR and CT studies in 10 patients with PACs to identify characteristic imaging features that facilitate their diagnosis.
Methods: MR and CT studies from 10 patients with PACs were reviewed retrospectively. In each case the PAC was characterized by lesion center, signal intensity or attenuation, adjacent petrous apex pneumatization, and its relationship to Meckel's cave. Intraoperative findings were reviewed in the three cases in which surgery was performed.
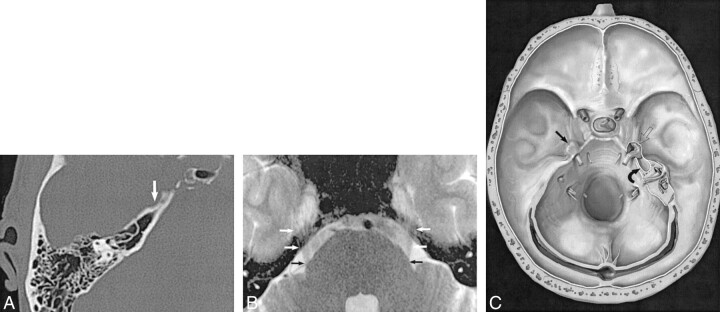
Results: All 10 patients had lobulated expansile cystic petrous apex lesions centered along the posterolateral margin of Meckel's cave. All cysts were contiguous with Meckel's cave. Three patients had bilateral PACs. Four patients had symptoms that could potentially be explained by the PAC, while findings in the other six were incidental observations. Three patients underwent surgery, during which two lesions were diagnosed as meningoceles while the third was diagnosed as an arachnoid cyst protruding through a dural defect.
Conclusion: PACs represent a protrusion of meninges and CSF from the posterolateral portion of Meckel's cave into the petrous apex, which is their characteristic imaging appearance. PACs are usually incidental but may be symptomatic. Surgical intervention should be approached cautiously and undertaken only when symptoms are clearly linked to the presence of this lesion.
Figures




References
-
- Moore K, Davidson H, Harnsberger H, Shelton C. A practical imaging approach to petrous apex lesions. IJNR Int J Neuroradiol 1999;5:166-184
-
- Cheung SW, Broberg TG, Jackler RK. Petrous apex arachnoid cyst: radiographic confusion with primary cholesteatoma. Am J Otol 1995;16:690-694 - PubMed
-
- Mulcahy MM, McMenomey SO, Talbot JM, Delashaw JB Jr. Congenital encephalocele of the medial skull base. Laryngoscope 1997;107:910-914 - PubMed
-
- Schick B, Draf W, Kahle G, Weber R, Wallenfang T. Occult malformations of the skull base. Arch Otolaryngol Head Neck Surg 1997;123:77-80 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous