

Loss of CDX2 expression and microsatellite instability are prominent features of large cell minimally differentiated carcinomas of the colon
- PMID: 11733373
- PMCID: PMC1850596
- DOI: 10.1016/S0002-9440(10)63074-X
Loss of CDX2 expression and microsatellite instability are prominent features of large cell minimally differentiated carcinomas of the colon
Abstract
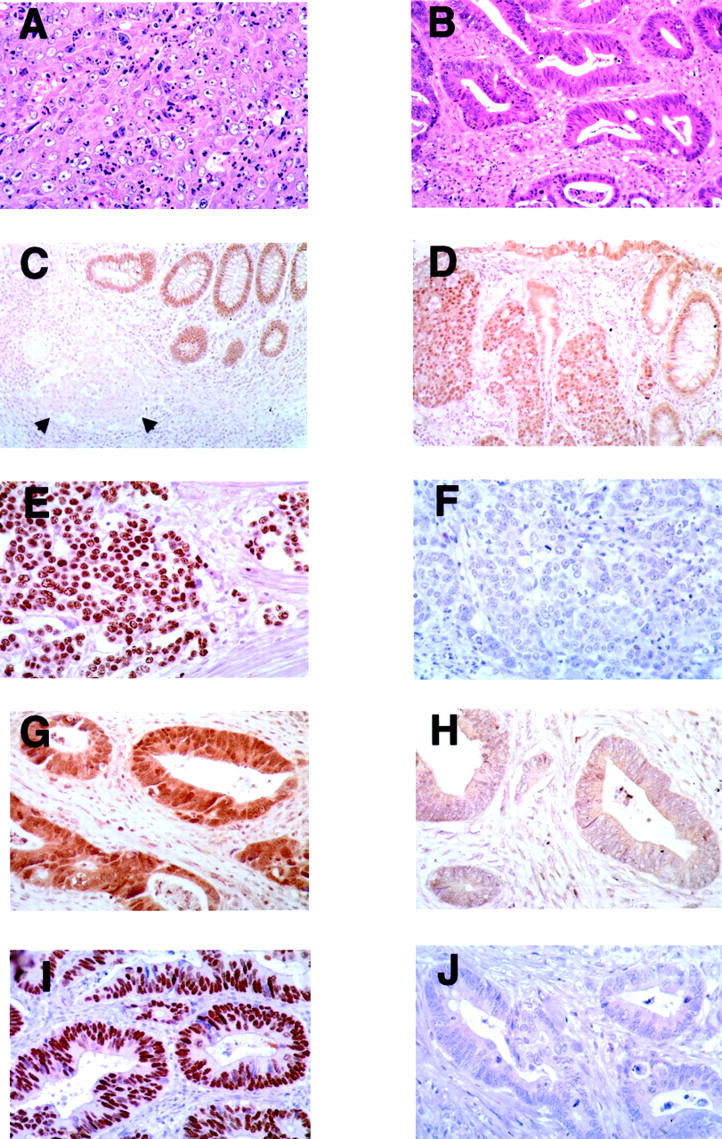
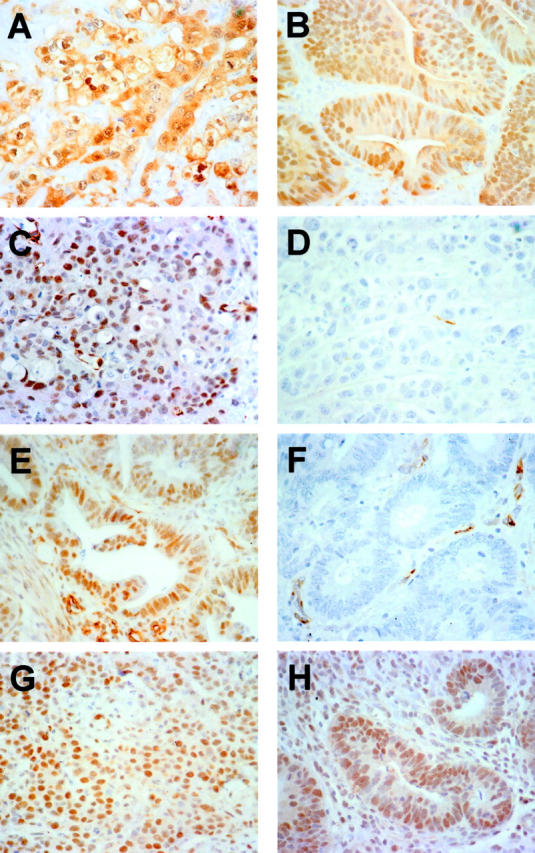
Most large bowel cancers are moderately to well-differentiated adenocarcinomas comprised chiefly or entirely of glands lined by tall columnar cells. We have identified a subset of poorly differentiated colon carcinomas with a distinctive histopathological appearance that we term large cell minimally differentiated carcinomas (LCMDCs). These tumors likely include a group of poorly differentiated carcinomas previously described by others as medullary adenocarcinomas. To better understand the pathogenesis of these uncommon neoplasms, we compared molecular features of 15 LCMDCs to those present in 25 differentiated adenocarcinomas (DACs) of the colon. Tumors were examined for alterations commonly seen in typical colorectal carcinomas, including increased p53 and beta-catenin immunoreactivity, K-ras gene mutations, microsatellite instability, and loss of heterozygosity of markers on chromosomes 5q, 17p, and 18q. In addition, tumors were evaluated by immunohistochemistry for CDX2, a homeobox protein whose expression in normal adult tissues is restricted to intestinal and colonic epithelium. Markedly reduced or absent CDX2 expression was noted in 13 of 15 (87%) LCMDCs, whereas only 1 of the 25 (4%) DACs showed reduced CDX2 expression (P < 0.001). Nine of 15 (60%) LCMDCs had the high-frequency microsatellite instability phenotype, but only 2 of 25 (8%) DACs had the high-frequency microsatellite instability phenotype (P = 0.002). Our findings provide support for the hypothesis that the molecular pathogenesis of LCMDCs is distinct from that of most DACs. CDX2 alterations and DNA mismatch repair defects have particularly prominent roles in the development of LCMDCs.
Figures
References
-
- Jessurun J, Romero-Guadarrama M, Manivel JC: Medullary adenocarcinoma of the colon: clinicopathologic study of 11 cases. Hum Pathol 1999, 30:843-848 - PubMed
-
- Reyes CV, Siddiqui MT: Anaplastic carcinoma of the colon: clinicopathologic study of eight cases of a poorly recognized lesion. Ann Diag Pathol 1997, 1:19-25 - PubMed
-
- Sugao Y, Yao T, Kubo C, Tsuneyoshi M: Improved prognosis of solid-type poorly differentiated colorectal adenocarcinoma: a clinicopathological and immunohistochemical study. Histopathology 1997, 31:123-133 - PubMed
-
- Kawabata Y, Tomita N, Monden T, Ohue M, Ohnishi T, Sasaki M, Sekimoto M, Sakita I, Tamaki Y, Takahashi J, Yagyu T, Mishima H, Kikkawa N, Monden M: Molecular characteristics of poorly differentiated adenocarcinoma and signet-ring-cell carcinoma of colorectum. Int J Cancer 1999, 84:33-38 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
