

Short-cycle structured intermittent treatment of chronic HIV infection with highly active antiretroviral therapy: effects on virologic, immunologic, and toxicity parameters
- PMID: 11734634
- PMCID: PMC65000
- DOI: 10.1073/pnas.261568398
Short-cycle structured intermittent treatment of chronic HIV infection with highly active antiretroviral therapy: effects on virologic, immunologic, and toxicity parameters
Abstract
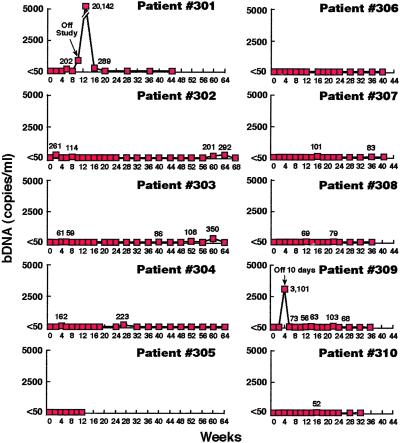
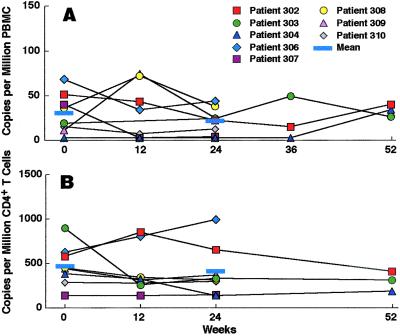
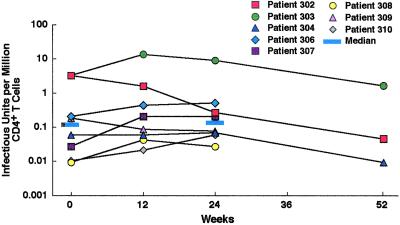
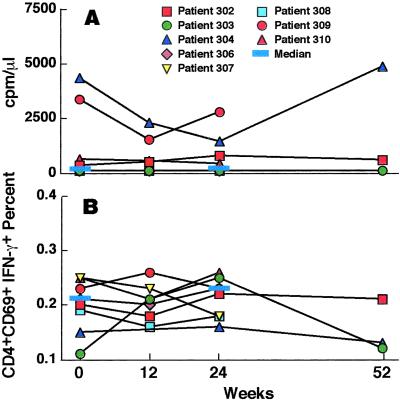
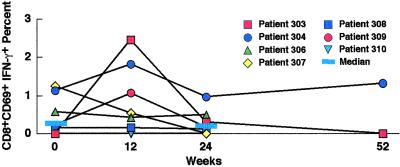
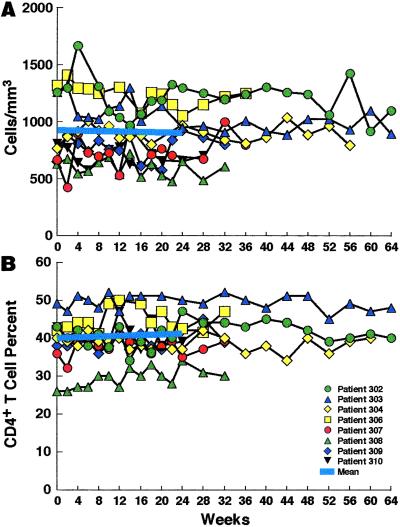
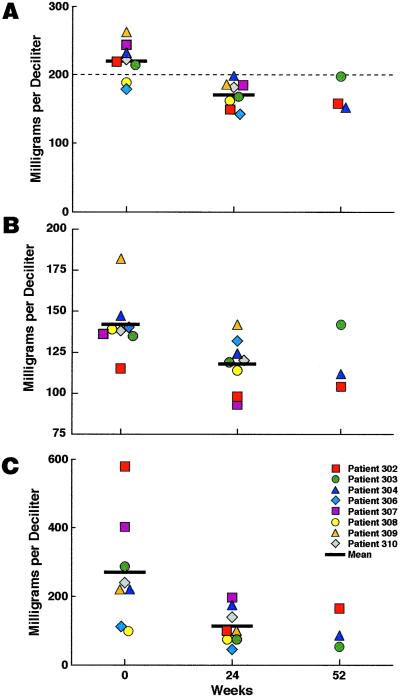
Although continuous highly active antiretroviral therapy (HAART) is effective for many HIV-infected patients, it can be toxic and prohibitive in cost. By decreasing the total amount of time patients receive medications, intermittent HAART could reduce toxicity and cost. Therefore, we initiated a pilot study in which 10 HIV-infected individuals receiving effective therapy that resulted in levels of HIV RNA <50 copies per ml of plasma and CD4(+) T cell counts >300 cells per mm(3) of whole blood received repeated cycles of 7 days on HAART followed by 7 days off of HAART. Patients maintained suppression of plasma viremia for 32-68 weeks. There was no significant increase in HIV proviral DNA or replication-competent HIV in peripheral CD4(+) T cells or HIV RNA in peripheral blood or lymph node mononuclear cells. There was no significant change in CD4(+) T cell counts, no significant increase in CD4(+) or CD8(+) T cells expressing activation markers or producing IFN-gamma in response to HIV, no increase in CD4(+) T cell proliferation to p24 antigen, and no evidence for the development of resistance to HAART medications. There was a significant decrease in serum cholesterol and triglyceride levels. Thus, in this proof-of-concept study, short-cycle intermittent HAART maintained suppression of plasma viremia as well as HIV replication in reservoir sites while preserving CD4(+) T cell counts. In addition, there was a decrease in serum cholesterol and triglyceride levels. Intermittent therapy may be an important strategy to reduce cost and toxicity for HIV-infected individuals.
Figures

References
-
- Centers for Disease Control and Prevention. HIV/AIDS Surveillance Report. 2000;12:1–44.
-
- Natarajan V, Bosche M, Metcalf J A, Ward D J, Lane H C, Kovacs J A. Lancet. 1999;353:119–120. - PubMed
-
- Furtado M R, Callaway D S, Phair J P, Kunstman K J, Stanton J L, Macken C A, Perelson A S, Wolinsky S M. N Engl J Med. 1999;340:1614–1622. - PubMed
-
- Zhang L, Ramratnam B, Tenner-Racz K, He Y, Vesanen M, Lewin S, Talal A, Racz P, Perelson A S, Korber B T, Markowitz M, Ho D D. N Engl J Med. 1999;340:1605–1613. - PubMed
-
- Behrens G, Dejam A, Schmidt H, Balks H J, Brabant G, Korner T, Stoll M, Schmidt R E. AIDS. 1999;13:F63–F70. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
