

T cell infiltration of the prostate induced by androgen withdrawal in patients with prostate cancer
- PMID: 11734652
- PMCID: PMC64722
- DOI: 10.1073/pnas.251140998
T cell infiltration of the prostate induced by androgen withdrawal in patients with prostate cancer
Abstract
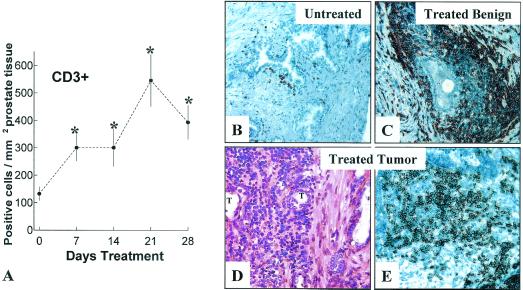
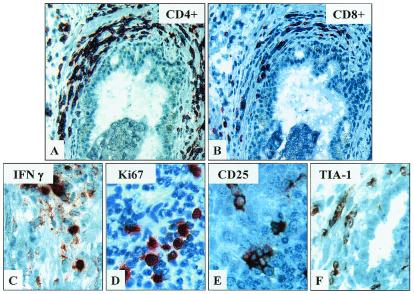
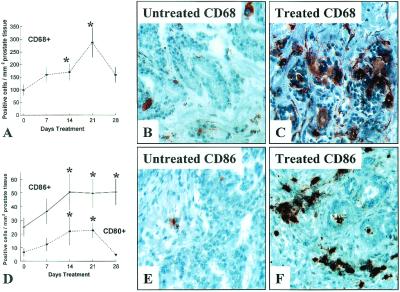
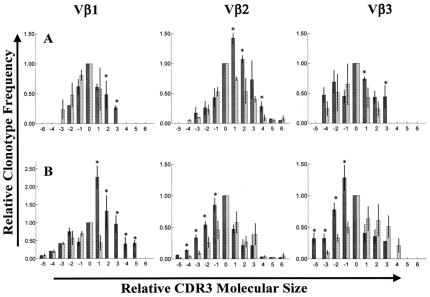
Manipulations capable of breaking host tolerance to induce tissue-specific T cell-mediated inflammation are of central importance to tumor immunotherapy and our understanding of autoimmunity. We demonstrate that androgen ablative therapy induces profuse T cell infiltration of benign glands and tumors in human prostates. T cell infiltration is readily apparent after 7-28 days of therapy and is comprised predominantly of a response by CD4+ T cells and comparatively fewer CD8+ T cells. Also, T cells within the treated prostate exhibit restricted TCR Vbeta gene usage, consistent with a local oligoclonal response. Recruitment/activation of antigen-presenting cells in treated prostate tissues may contribute to local T cell activation. The induction of T cell infiltration in prostate tissues treated with androgen ablation may have implications for the immunotherapeutic treatment of prostate cancer as well as other hormone-sensitive malignancies, including breast carcinoma.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
