

Responsible prescribing for upper respiratory tract infections
- PMID: 11735633
- PMCID: PMC7099238
- DOI: 10.2165/00003495-200161140-00004
Responsible prescribing for upper respiratory tract infections
Abstract
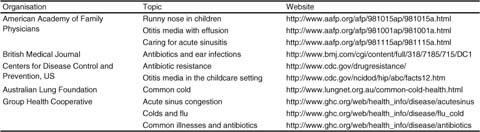
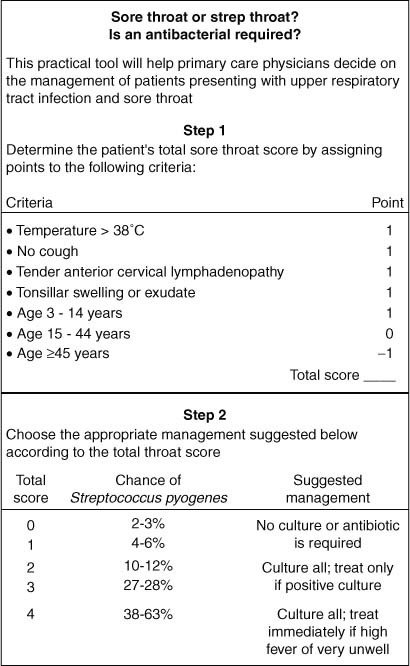
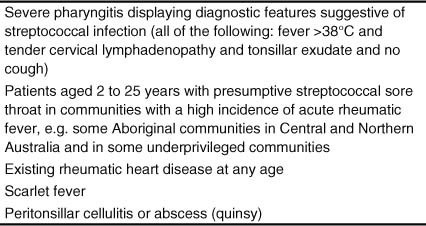
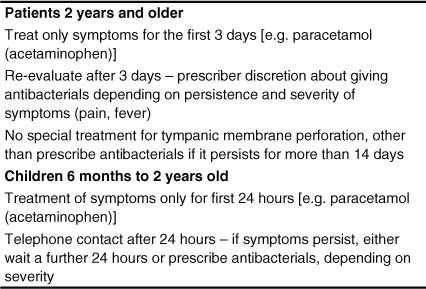
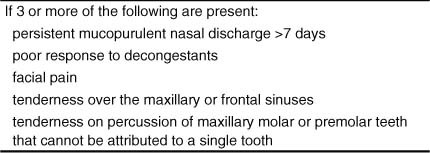
Upper respiratory tract infections (URTIs) are responsible for a large amount of community antibacterial use worldwide. Recent systematic reviews have demonstrated that most URTIs resolve naturally, even when bacteria are the cause. The high consumer expectation for antibacterials in URTIs requires intervention by the general practitioner and a number of useful strategies have been developed. Generic strategies, including eliciting patient expectations, avoiding the term 'just a virus', providing a value-for-money consultation, providing verbal and written information, empowering patients, conditional prescribing, directed education campaigns, and emphasis on symptomatic treatments, should be used as well as discussion of alternative medicines when relevant. The various conditions have differing rates of bacterial infection and require different approaches. For acute rhinitis, laryngitis and tracheitis, viruses are the only cause and, therefore, antibacterials are never required. In acute sore throat (pharyngitis) Streptococcus pyogenes is the only important bacterial cause. A scoring system can help to increase the likelihood of distinguishing a streptococcal as opposed to viral infection, or alternatively patients should be given antibacterials only if certain conditions are fulfilled. Strategies for treating acute otitis media vary in different countries. Most favour the strategy of prescribing antibacterials only when certain criteria are fulfilled, delaying antibacterial prescribing for at least 24 hours. In otitis media with effusion, on the other hand, there is no primary role for antibacterials, as the condition resolves naturally in almost all patients aged >3 months. Detailed strategies for acute sinusitis have not been worked out but restricting antibacterial prescribing to certain clinical complexes is currently recommended by several authorities because of the high natural resolution rate.
Figures

Similar articles
-
Predictors of broad-spectrum antibiotic prescribing for acute respiratory tract infections in adult primary care.JAMA. 2003 Feb 12;289(6):719-25. doi: 10.1001/jama.289.6.719. JAMA. 2003. PMID: 12585950
-
Association between antibiotic prescribing and visit duration in adults with upper respiratory tract infections.Clin Ther. 2003 Sep;25(9):2419-30. doi: 10.1016/s0149-2918(03)80284-9. Clin Ther. 2003. PMID: 14604741
-
Antibiotic choice in UK general practice: rates and drivers of potentially inappropriate antibiotic prescribing.J Antimicrob Chemother. 2019 Nov 1;74(11):3371-3378. doi: 10.1093/jac/dkz345. J Antimicrob Chemother. 2019. PMID: 31430365
-
Antimicrobial treatment of ENT infections.Infect Dis Now. 2023 Nov;53(8S):104785. doi: 10.1016/j.idnow.2023.104785. Epub 2023 Sep 18. Infect Dis Now. 2023. PMID: 37730165 Review.
-
Homeopathy in the Age of Antimicrobial Resistance: Is It a Viable Treatment for Upper Respiratory Tract Infections?Homeopathy. 2018 May;107(2):99-114. doi: 10.1055/s-0037-1621745. Epub 2018 Feb 5. Homeopathy. 2018. PMID: 29767829 Review.
References
-
- World Health Organization. Global strategy for containment of antimicrobial resistance —draft [online]. Available from URL: http://www.who.int/emc/globalstrategy/strategy.html [Accessed 2000 Sep]
-
- Collignon PJ, Turnidge JD. Antibiotic resistance in Streptococcus pneumoniae. Med J Aust. 2000;173:S58–64. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
