

Single-center analysis of early recurrence of nephrotic syndrome following renal transplantation in children
- PMID: 11737765
- PMCID: PMC1350578
- DOI: 10.1034/j.1399-3046.2001.t01-2-00024.x
Single-center analysis of early recurrence of nephrotic syndrome following renal transplantation in children
Abstract
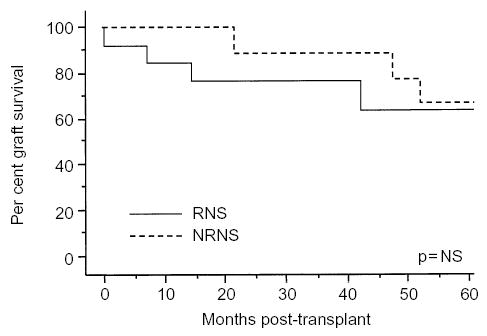
Recurrence of nephrotic syndrome (NS) after transplantation (Tx) occurs in 20-50% of renal transplant recipients, with a median time to recurrence of 14 days and a 50% rate of graft loss. We performed a retrospective analysis of 22 pediatric patients with NS who received renal transplants at the Children's Hospital, Boston, between 1982 and 1999. During the first 14 days following Tx, 13 (59%) patients developed clinical recurrent nephrotic syndrome (RNS). RNS developed in 50% of living donor recipients and in 70% of cadaveric donor recipients (p= non-significant). Seven of the 13 patients with RNS were treated with plasmapheresis, while six received standard immunosuppressive induction therapy only. Two of the seven treated patients and one of the six untreated patients lost their grafts to RNS, yielding a total RNS graft loss rate of 23%. However, patients with RNS who achieved remission had significantly higher cumulative graft survival at 5 yr than did RNS patients who did not achieve remission (p< 0.001). Overall cumulative graft survival at 5 yr was not significantly different between the two groups: 67% in those with non-recurrent nephrotic syndrome (NRNS) vs. 64% in those with RNS, p= non-significant. We conclude that successful reversal of early RNS improves long-term graft survival in pediatric RNS. Multi-center studies are sorely needed to develop novel, less toxic therapies for native and recurrent NS.
Figures

References
-
- McDonald R, Donaldson L, Emmett L, Tejani A. A decade of living donor transplantation in North American Children. The 1998 Annual Report of the North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) Pediatr Transpl. 2000;4:221. - PubMed
-
- Kashtan C, McEnery P, Tejani A, Stablein D. Renal allograft survival accordingto primarydiagnosis: a report of the North American Pediatric Renal Transplant Cooperative Study. Pediatr Nephrol. 1995;9:679. - PubMed
-
- Senggutuvan P, Cameron J, Hartley R, et al. Recurrence of focal segmental glomerulosclerosis in transplanted kidneys: analysis of incidence and risk factors in 59 allografts. Pediatr Nephrol. 1990;4:21. - PubMed
-
- Tejani A, Stablein D. Recurrence of focal segmental glomerulosclerosis posttransplantation: a special report of the North American Pediatric Renal Transplant Cooperative Study. J Am Soc Nephrol. 1992;2 (Suppl 3):S256. - PubMed
-
- Dall’Amico R, Ghiggeri G, Carraro M, et al. Prediction and treatment of recurrent focal segmental glomerulosclerosis after renal transplantation in children. Am J Kidney Dis. 1999;34:1048. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
