

Decreased bone mineral density in Prader-Willi syndrome: comparison with obese subjects
- PMID: 11745993
- PMCID: PMC5157204
Decreased bone mineral density in Prader-Willi syndrome: comparison with obese subjects
Abstract
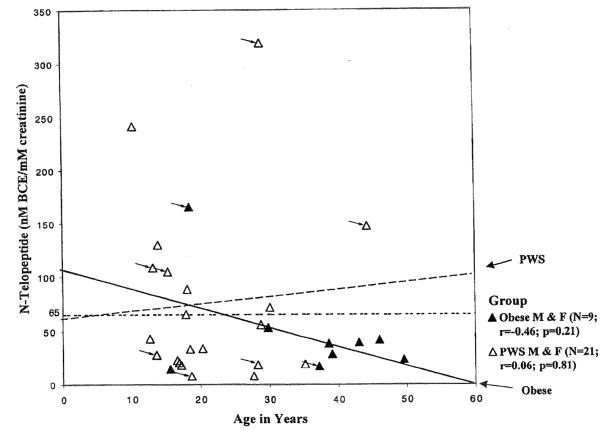
Bone density, anthropometric data, and markers of bone turnover were collected on 21 subjects diagnosed with Prader-Willi syndrome (PWS) and compared with 9 subjects with obesity of unknown cause. In addition, urinary N-telopeptide levels were obtained in all subjects. N-telopeptides are the peptide fragments of type I collagen, the major bone matrix material. During periods of active bone degradation or high bone turnover, high levels of N-telopeptides are excreted in the urine. However, no significant difference was detected in the urinary N-telopeptide levels when corrected for creatinine excretion (raw or transformed data) between our subjects with obesity or PWS and the observed effect size of the between-group difference was small. Although N-telopeptide levels were higher but not significantly different in the subjects with PWS compared with obese controls, the subjects with PWS had significantly decreased total bone and spine mineral density and total bone mineral content (all P < 0.001). No differences in N-telopeptide levels or bone mineral density were observed between subjects with PWS and chromosome 15q deletion or maternal disomy. Thus, decreased bone mineral density in subjects with PWS may relate to the lack of depositing bone mineral during growth when bones are becoming more dense (e.g., during adolescence), possibly because of decreased production of sex or growth hormones and/or long-standing hypotonia. It may not be caused by loss, or active degradation, of bone matrix measurable by the methods described in this study further supporting the possible need for hormone therapy during adolescence.
Copyright 2001 Wiley-Liss, Inc.
Figures




References
-
- Borenstein M, Rothstein H, Cohen J. Power and precision. Teaneck, NJ: Biostat; 1997.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical