

Hepatic cavernous hemangioma in cirrhotic liver: imaging findings
- PMID: 11752953
- PMCID: PMC2718199
- DOI: 10.3348/kjr.2000.1.4.185
Hepatic cavernous hemangioma in cirrhotic liver: imaging findings
Abstract
Objective: To document the imaging findings of hepatic cavernous hemangioma detected in cirrhotic liver.
Materials and methods: The imaging findings of 14 hepatic cavernous hemangiomas in ten patients with liver cirrhosis were retrospectively analyzed. A diagnosis of hepatic cavernous hemangioma was based on the findings of two or more of the following imaging studies: MR, including contrast-enhanced dynamic imaging (n = 10), dynamic CT (n = 4), hepatic arteriography (n = 9), and US (n = 10).
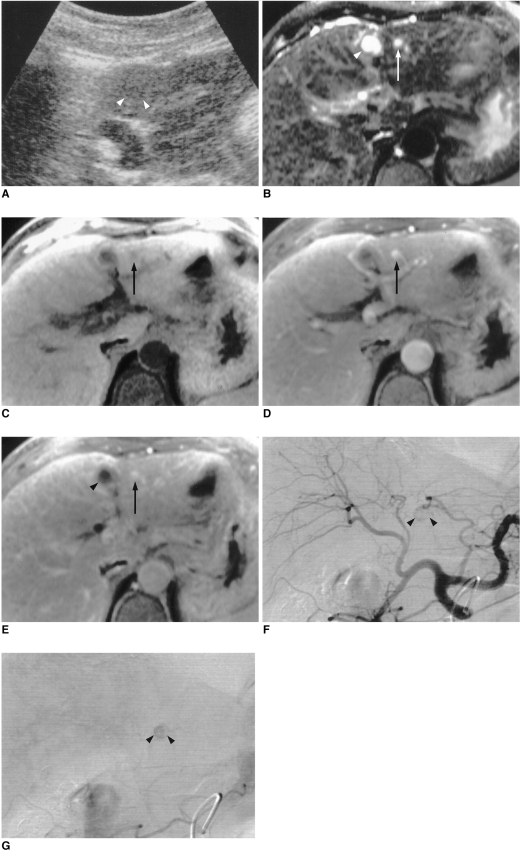
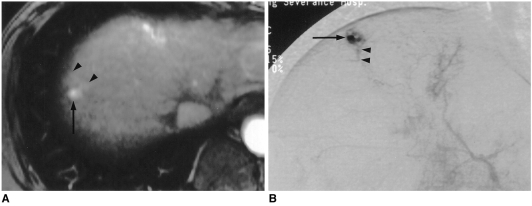
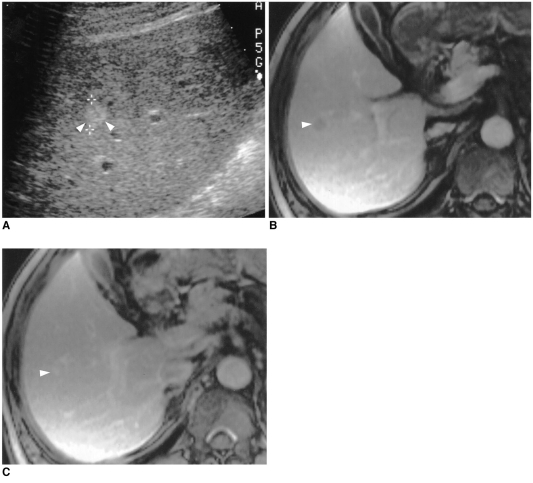
Results: The mean size of the 14 hepatic hemangiomas was 0.9 (range, 0.5-1.5) cm in the longest dimension. In 11 of these (79%), contrast-enhanced dynamic CT and MR imaging showed rapid contrast enhancement of the entire lesion during the early phase, and hepatic arteriography revealed globular enhancement and rapid filling-in. On contrast-enhanced MR images, three lesions (21%) showed partial enhancement until the 5-min delayed phases. US indicated that while three slowly enhancing lesions were homogeneously hyperechoic, 9 (82%) of 11 showing rapid enhancement were not delineated.
Conclusion: The majority of hepatic cavernous hemangiomas detected in cirrhotic liver are small in size, and in many, hepatic arteriography and/or contrast-enhanced dynamic CT and MR imaging demonstrates rapid enhancement. US, however, fails to distinguish a lesion of this kind from its cirrhotic background.
Figures
References
-
- Itai Y, Ohnishi S, Ohtomo K, Kokubo T, Imawari M, Atomi Y. Hepatic cavernous hemangioma in patients at high risk for liver cancer. Acta Radiol. 1987;28:697–701. - PubMed
-
- Hanafusa K, Ohashi I, Himeno Y, Suzuki S, Shibuya H. Hepatic hemangioma: findings with two-phase CT. Radiology. 1995;196:465–469. - PubMed
-
- Takayasu K, Moriyama N, Shima Y, et al. Atypical radiographic findings in hepatic cavernous hemangioma: correlation with histologic features. AJR. 1986;146:1149–1153. - PubMed
-
- Moody AR, Wilson SR. Atypical hepatic hemangioma: a suggestive sonographic morphology. Radiology. 1993;188:413–417. - PubMed
-
- Freeny PC, Vimont TR, Barnett DC. Cavernous hemangioma of the liver: ultrasonography, arteriography, and computed tomography. Radiology. 1979;132:143–148. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
