

Preoperative galactose elimination capacity predicts complications and survival after hepatic resection
- PMID: 11753045
- PMCID: PMC1422398
- DOI: 10.1097/00000658-200201000-00010
Preoperative galactose elimination capacity predicts complications and survival after hepatic resection
Abstract
Objective: To analyze a single center's 6-year experience with 258 consecutive patients undergoing major hepatic resection for primary or secondary malignancy of the liver, and to examine the predictive value of preoperative liver function assessment.
Summary background data: Despite the substantial improvements in diagnostic and surgical techniques that have made liver surgery a safer procedure, careful patient selection remains mandatory to achieve good results in patients with hepatic tumors.
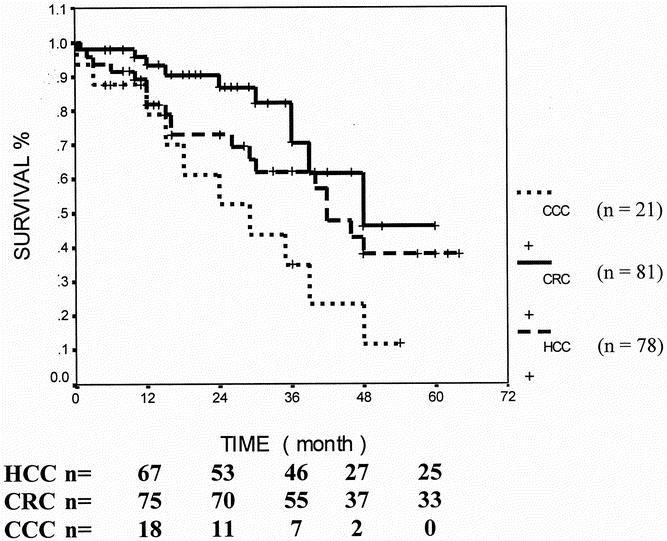
Methods: In this prospective study, 258 patients undergoing hepatic resection were enrolled: 111 for metastases, 78 for hepatocellular carcinoma (HCC), 21 for cholangiocellular carcinoma, and 48 for other primary hepatic tumors. One hundred fifty-eight patients underwent segment-oriented liver resection, including hemihepatectomies, and 100 had subsegmental resections. Thirty-two clinical and biochemical parameters were analyzed, including liver function assessment by the galactose elimination capacity (GEC) test, a measure of hepatic functional reserve, to predict postoperative (60-day) rates of death and complications and long-term survival. All variables were determined within 5 days before surgery. Data were subjected to univariate and multivariate analysis for two patient subgroups (HCC and non-HCC). The cutoffs for GEC in both groups were predefined. Long-term survival (>60 days) was subjected to Kaplan-Meier analysis and the Cox proportional hazard model.
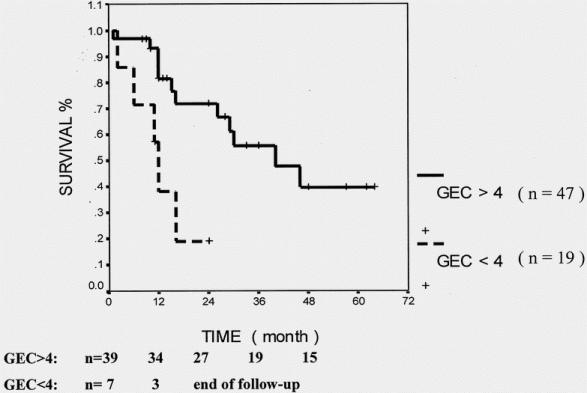
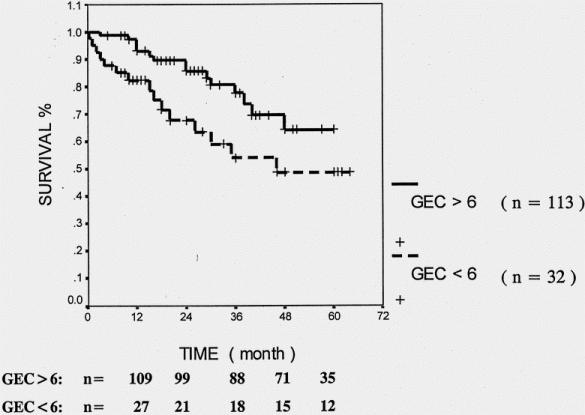
Results: In the entire group of 258 patients, a GEC less than 6 mg/min/kg was the only preoperative biochemical parameter that predicted postoperative complications and death by univariate and stepwise regression analysis. A GEC of more than 6 mg/min/kg was also significantly associated with longer survival. This predictive value could also be shown in the subgroup of 180 patients with tumors other than HCC. In the subgroup of 78 patients with HCC, a GEC less than 4 mg/min/kg predicted postoperative complications and death by univariate and stepwise regression analysis. Further, a GEC of more than 4 mg/min/kg was also associated with longer survival.
Conclusions: This prospective study establishes the preoperative determination of the hepatic reserve by GEC as a strong independent and valuable predictor for short- and long-term outcome in patients with primary and secondary hepatic tumors undergoing resection.
Figures
References
-
- El-Serag HB, Mason AC. Rising incidence of hepatocellular carcinoma in the United States. N Engl J Med 1999; 340: 745–750. - PubMed
-
- Michel J, Suc B, Montpeyroux F, et al. Liver resection or transplantation for hepatocellular carcinoma? Retrospective analysis of 215 patients with cirrhosis. J Hepatol 1997; 26: 1274–1280. - PubMed
-
- Marsh JW, Dvorchik I, Iwatsuki S. Liver transplantation in the treatment of hepatocellular carcinoma. J Hepatobiliary Pancreat Surg 1998; 5: 24–28. - PubMed
-
- Fong Y, Salo J. Surgical therapy of hepatic colorectal metastasis. Semin Oncol 1999; 26: 514–523. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
