

Differential effect of angiotensin II on blood circulation in the renal medulla and cortex of anaesthetised rats
- PMID: 11773324
- PMCID: PMC2290021
- DOI: 10.1113/jphysiol.2001.012921
Differential effect of angiotensin II on blood circulation in the renal medulla and cortex of anaesthetised rats
Abstract
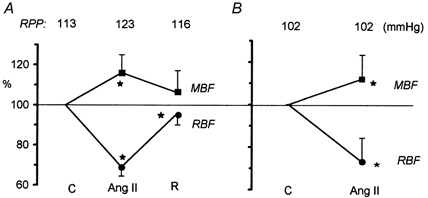
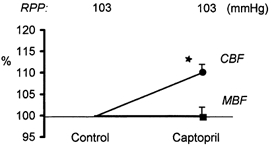
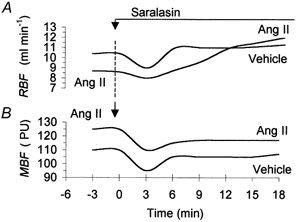
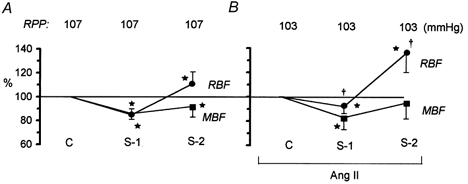
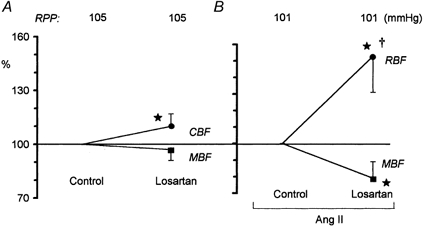
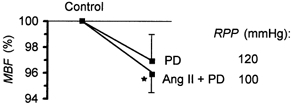
The renal medulla is sensitive to hypoxia, and a depression of medullary circulation, e.g. in response to angiotensin II (Ang II), could endanger the function of this zone. Earlier data on Ang II effects on medullary vasculature were contradictory. The effects of Ang II on total renal blood flow (RBF), and cortical and medullary blood flow (CBF and MBF: by laser-Doppler flux) were studied in anaesthetised rats. Ang II infusion (30 ng kg(-1) min(-1) i.v.) decreased RBF 27 +/- 2 % (mean +/- S.E.M.), whereas MBF increased 12 +/- 2 % (both P < 0.001). Non-selective blockade of Ang II receptors with saralasin (3 microg kg(-1) min(-1) i.v.) increased RBF 12 +/- 2 % and decreased MBF 8 +/- 2 % (P < 0.001). Blockade of AT(1) receptors with losartan (10 mg kg(-1)) increased CBF 10 +/- 2 % (P < 0.002) and did not change MBF. Losartan given during Ang II infusion significantly increased RBF (53 +/- 7 %) and decreased MBF (27 +/- 7 %). Blockade of AT(2) receptors with PD 123319 (50 microg kg(-1) min(-1) i.v.) did not change CBF or MBF. Intramedullary infusion of PD 123319 (10 microg min(-1)) superimposed on intravenous Ang II infusion did not change RBF, but slightly decreased MBF (4 +/- 2 %, P < 0.05). We conclude that in anaesthetised surgically prepared rats, exogenous or endogenous Ang II may not depress medullary circulation. In contrast to the usual vasoconstriction in the cortex, vasodilatation was observed, possibly related to secondary activation of vasodilator paracrine agents rather than to a direct action via AT(2) receptors.
Figures
References
-
- Arendshorst WJ, Brännström K, Ruan X. Action of angiotensin II on the renal microvasculature. Journal of the American Society of Nephrology. 1999;10:S149–161. - PubMed
-
- Cowley AW. Role of the renal medulla in volume and arterial blood pressure regulation. American Journal of Physiology. 1997;273:R1–15. - PubMed
-
- Csikós T, Chung O, Unger Th. Receptors and their classification: Focus on angiotensin II and the AT2 receptor. Journal of Human Hypertension. 1998;12:311–318. - PubMed
-
- Cupples WA, Sonnenberg H. Renal medullary plasma flow rate and reabsorption of salt and water from inner medullary collecting duct. Canadian Journal of Physiology and Pharmacology. 1987;65:2415–2421. - PubMed
-
- de Gasparo M, Siragy HM. The AT2 receptor: fact, fancy and fantasy. Regulatory Peptides. 1999;81:11–24. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous