

Growth factors in idiopathic pulmonary fibrosis: relative roles
- PMID: 11806848
- PMCID: PMC64811
- DOI: 10.1186/rr162
Growth factors in idiopathic pulmonary fibrosis: relative roles
Abstract
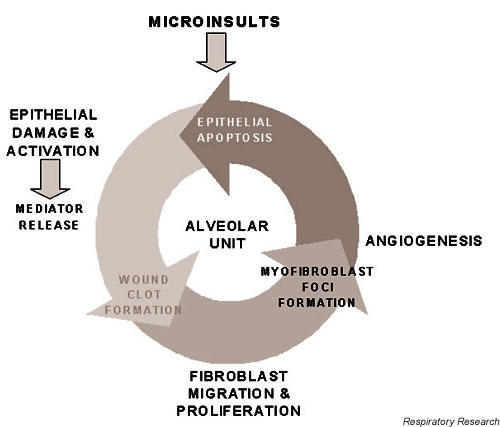
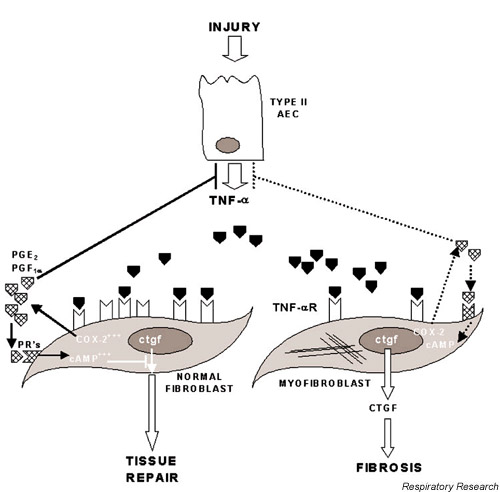
Treatment of idiopathic pulmonary fibrosis patients has evolved very slowly; the fundamental approach of corticosteroids alone or in combination with other immunosuppressive agents has had little impact on long-term survival. The continued use of corticosteroids is justified because of the lack of a more effective alternative. Current research indicates that the mechanisms driving idiopathic pulmonary fibrosis reflect abnormal, dysregulated wound healing within the lung, involving increased activity and possibly exaggerated responses by a spectrum of profibrogenic growth factors. An understanding of the roles of these growth factors, and the way in which they modulate events at cellular level, could lead to more targeted therapeutic strategies, improving patients' quality of life and survival.
Figures

References
-
- The American Thoracic Society and the European Respiratory Society Idiopathic pulmonary fibrosis: Diagnosis and treatment. International consensus statement. Am J Respir Crit Care Med. 2000;161:646–664. - PubMed
-
- Flaherty KR, Toews GB, Lynch JP, Kazerooni EA, Gross BH, Strawderman RL, Hariharan K, Flint A, Martinez FJ. Steroids in pulmonary fibrosis: A perspective assessment of adverse reactions, response to therapy, and survival. Am J Med. 2001;110:278–282. doi: 10.1016/S0002-9343(00)00711-7. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
