

Risk of small bowel obstruction after the ileal pouch-anal anastomosis
- PMID: 11807359
- PMCID: PMC1422415
- DOI: 10.1097/00000658-200202000-00007
Risk of small bowel obstruction after the ileal pouch-anal anastomosis
Abstract
Objective: To determine the incidence of small bowel obstruction (SBO), to identify risk factors for its development, and to determine the most common sites of adhesions causing SBO in patients undergoing ileal pouch-anal anastomosis (IPAA).
Methods: All patients undergoing IPAA at Mount Sinai Hospital were included. Data were obtained from the institution's database, patient charts, and a mailed questionnaire. SBO was based on clinical, radiologic, and surgical findings. Early SBO was defined as a hospital stay greater than 10 or 14 days because of delayed bowel function, or need for reoperation or readmission for SBO within 30 days. All patients readmitted after 30 days with a discharge diagnosis of SBO were considered to have late SBO.
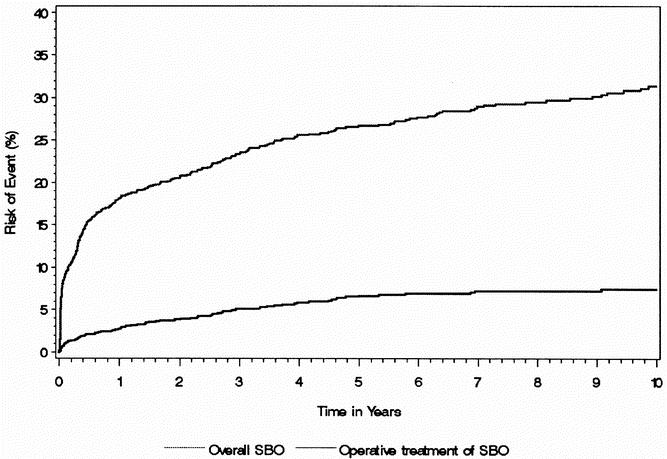
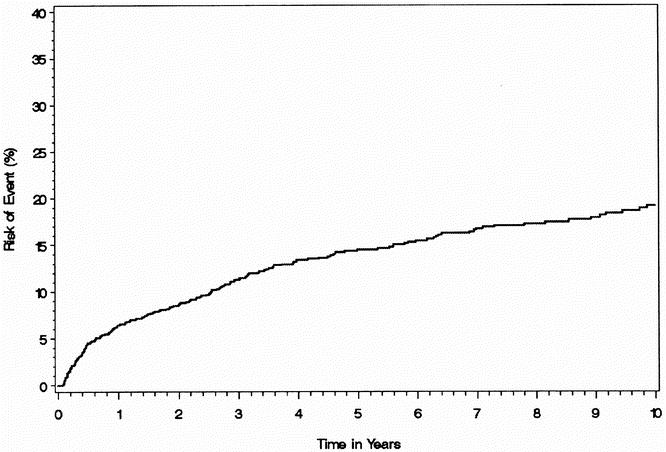
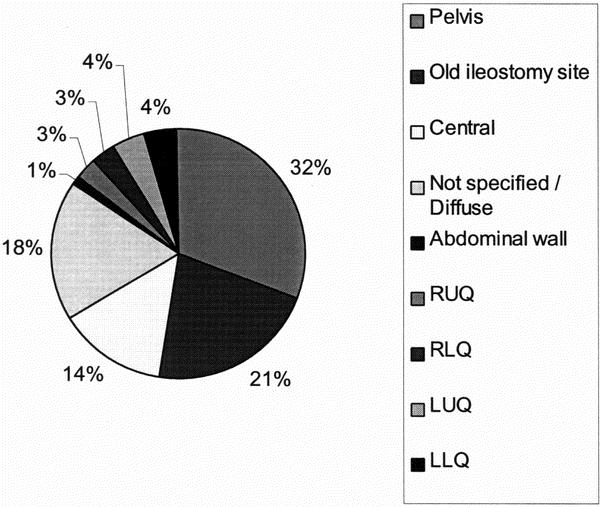
Results: Between 1981 and 1999, 1,178 patients underwent IPAA (664 men, 514 women; mean age 40.7 years). A total of 351 episodes of SBO were documented in 272 (23%) patients during a mean follow-up of 8.7 years (mean 1.29 episodes/patient). Fifty-four patients had more than one SBO. One hundred fifty-four (44%) of the SBOs occurred in the first 30 days; 197 (56%) were late SBOs. The cumulative risk of SBO was 8.7% at 30 days, 18.1% at 1 year, 26.7% at 5 years, and 31.4% at 10 years. The need for surgery for SBO was 0.8% at 30 days, 2.7% at 1 year, 6.7% at 5 years, and 7.5% at 10 years. In patients requiring laparotomy, the obstruction was most commonly due to pelvic adhesions (32%), followed by adhesions at the ileostomy closure site (21%). A multivariate analysis showed that when only late SBOs were considered, performance of a diverting ileostomy and pouch reconstruction both led to a significantly higher risk of SBO.
Conclusions: The risk of SBO after IPAA is high, although most do not require surgical intervention. Thus, strategies that reduce the risk of adhesions are warranted in this group of patients to improve patient outcome and decrease healthcare costs.
Figures
References
-
- Buckman RF, Woods M, Sargent L, et al. A unifying pathogenetic mechanism in the etiology of intraperitoneal adhesions. J Surg Res 1976; 20: 1–5. - PubMed
-
- Weibel MA, Majno G. Peritoneal adhesions and their relation to abdominal surgery. A postmortem study. Am J Surg 1973; 126: 345–353. - PubMed
-
- Wilson MS, Hawkswell J, McCloy RF. Natural history of adhesional small bowel obstruction: counting the cost. Br J Surg 1998; 85: 1294–1298. - PubMed
-
- Ivarsson ML, Holmdahl L, Franzen G, et al. Cost of bowel obstruction resulting from adhesions. Eur J Surg 1997; 163: 679–684. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
