

Risk factors for ileoanal J pouch-related septic complications in ulcerative colitis and familial adenomatous polyposis
- PMID: 11807360
- PMCID: PMC1422416
- DOI: 10.1097/00000658-200202000-00008
Risk factors for ileoanal J pouch-related septic complications in ulcerative colitis and familial adenomatous polyposis
Abstract
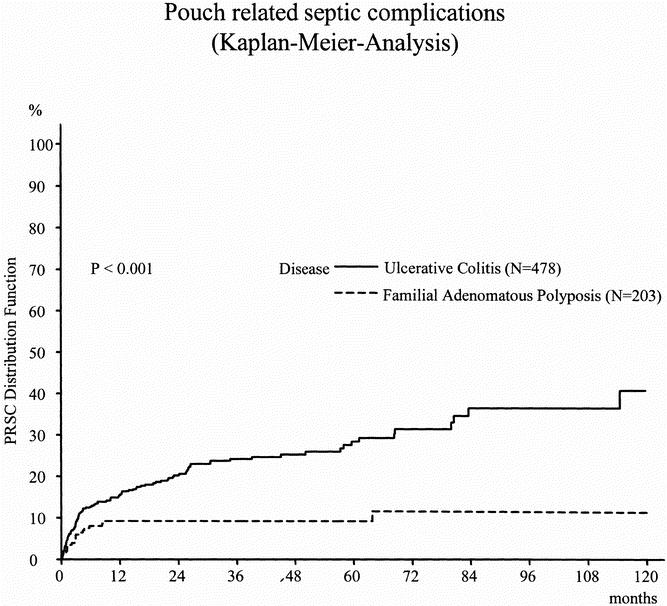
Objective: To analyze the association between pre- and perioperative factors and pouch-related septic complications (PRSC) in ulcerative colitis (UC) and in familial adenomatous polyposis (FAP) after ileal pouch-anal anastomosis (IPAA).
Summary background data: For patients with UC and FAP, IPAA is the surgical therapy of choice, but in some patients the outcome is compromised by PRSC.
Methods: A total of 706 consecutive patients (494 UC, 212 FAP) were assessed in a study aimed at identifying subgroups of patients who were at high risk for PRSC. The rate of PRSC was analyzed as a time-dependent function (Kaplan-Meier estimation). Patients with UC and FAP were stratified separately according to associated factors (age, sex, surgeon's experience, temporary ileostomy, colectomy before IPAA, anastomotic tension, and several factors specific for UC).
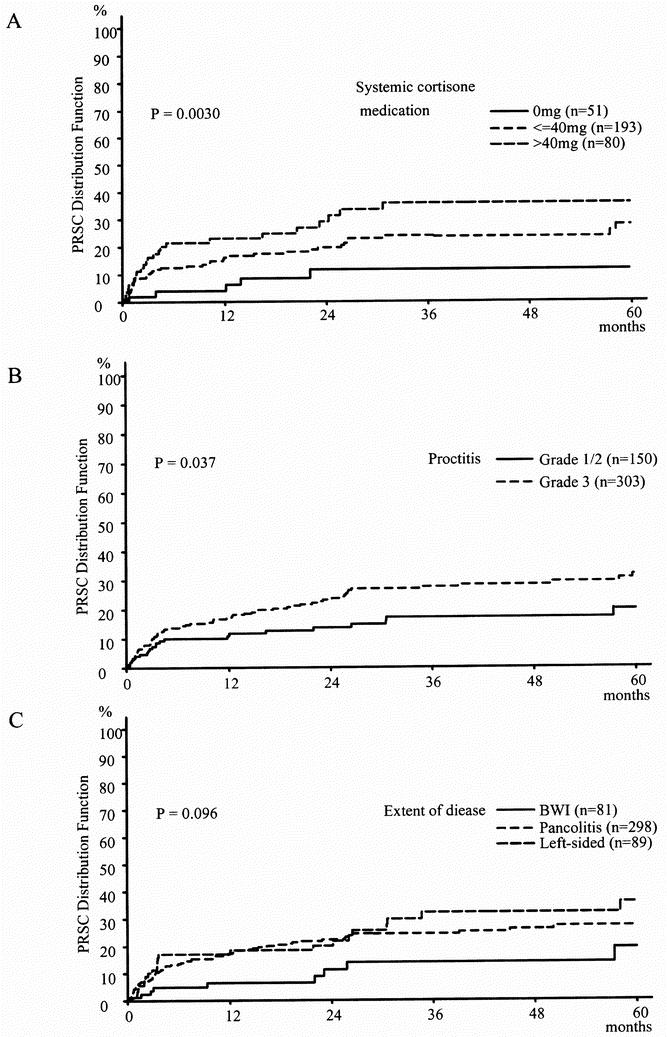
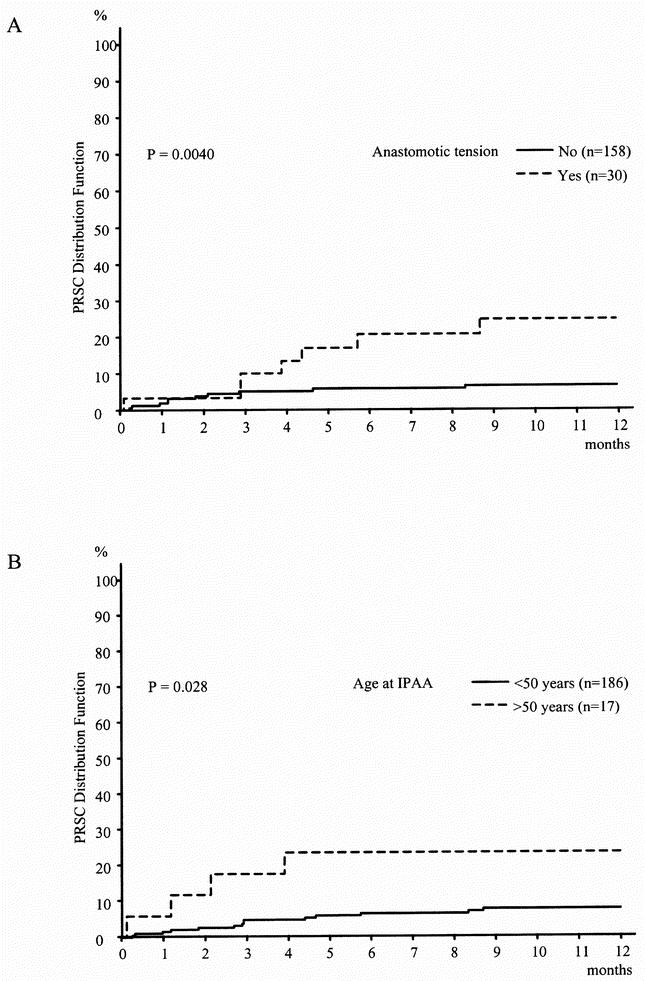
Results: In all, 131 (19.2%) patients had PRSC (23.4% UC, 9.4% FAP). In patients with UC, the estimated 1-year PRSC rate was 15.6% and the estimated 3-year PRSC rate was 24.2%. In patients with FAP, the estimated 1-year and 3-year PRSC rates were 9.2%. The difference between the estimated rates of PRSC was significant (P <.001). In the univariate analysis, patients with UC younger than 50 years, with severe proctitis, with preoperative hemoglobin levels less than 10 g/L, or receiving corticoid medication had a significantly higher risk for PRSC (P =.039, P =.037, P =.047, P =.003, respectively). Multivariate analysis showed that patients with UC receiving a systemic prednisolone-equivalent corticoid medication of more than 40 mg/day had a significantly greater risk of developing pouch-related complications than patients with UC receiving 1 to 40 mg/day and patients with UC who were not receiving corticoid medication (RR: 3.78, 2.25, 1, respectively, P <.001). Patients with FAP proved to have a significantly higher risk for PRSC in the univariate and multivariate analyses if anastomotic tension had occurred (RR 3.60, P =.0086).
Conclusions: Pouch-related septic complications occur as late complications and should therefore be considered in regular, specific long-term follow-up examinations. The authors identified significant risk factors for PRSC specific to patients with UC and FAP; these must be considered for each individual surgical strategy.
Figures
Similar articles
-
D-pouch: a modified ileal J-pouch for patients with ulcerative colitis and familial adenomatous polyposis.Tech Coloproctol. 2021 Nov;25(11):1209-1215. doi: 10.1007/s10151-021-02437-4. Epub 2021 Apr 7. Tech Coloproctol. 2021. PMID: 33826024
-
Does Age Affect Surgical Outcomes After Ileal Pouch-Anal Anastomosis in Children?J Surg Res. 2019 May;237:61-66. doi: 10.1016/j.jss.2019.01.004. Epub 2019 Jan 30. J Surg Res. 2019. PMID: 30710880
-
Restorative proctocolectomy with ileal pouch-anal anastomosis for ulcerative colitis and familial adenomatous polyposis: twenty years follow-up in 174 patients.Isr Med Assoc J. 2005 Jan;7(1):23-7. Isr Med Assoc J. 2005. PMID: 15658141
-
Current Status and Surgical Technique for Restorative Proctocolectomy with Ileal Pouch Anal Anastomosis.Balkan Med J. 2023 Jul 12;40(4):236-243. doi: 10.4274/balkanmedj.galenos.2023.2023-5-12. Epub 2023 Jun 23. Balkan Med J. 2023. PMID: 37350728 Free PMC article. Review.
-
Complications after proctocolectomy and ileal pouch-anal anastomosis in pediatric patients: A systematic review.J Pediatr Surg. 2019 Jul;54(7):1331-1339. doi: 10.1016/j.jpedsurg.2018.08.047. Epub 2018 Sep 19. J Pediatr Surg. 2019. PMID: 30291026
Cited by
-
Serum biochemical evaluation of patients with functional pouches ten to 20 years after restorative proctocolectomy.Int J Colorectal Dis. 2006 Oct;21(7):711-20. doi: 10.1007/s00384-005-0076-3. Epub 2006 Jan 26. Int J Colorectal Dis. 2006. PMID: 16437210
-
The effect of ageing on function and quality of life in ileal pouch patients: a single cohort experience of 409 patients with chronic ulcerative colitis.Ann Surg. 2004 Oct;240(4):615-21; discussion 621-3. doi: 10.1097/01.sla.0000141157.32234.9d. Ann Surg. 2004. PMID: 15383789 Free PMC article.
-
Associations between multiple immunosuppressive treatments before surgery and surgical morbidity in patients with ulcerative colitis during the era of biologics.Int J Colorectal Dis. 2019 Apr;34(4):699-710. doi: 10.1007/s00384-019-03253-x. Epub 2019 Jan 26. Int J Colorectal Dis. 2019. PMID: 30685791
-
Neutrophil dysfunction in steroid-overdosed patients with ulcerative colitis: potential relevance of macrophage migration inhibitory factor to increased postoperative morbidity.Surg Today. 2011 Nov;41(11):1504-11. doi: 10.1007/s00595-010-4505-8. Epub 2011 Oct 4. Surg Today. 2011. PMID: 21969153
-
Colectomy with ileostomy for severe ulcerative colitis-postoperative complications and risk factors.Int J Colorectal Dis. 2020 Mar;35(3):387-394. doi: 10.1007/s00384-019-03494-w. Epub 2019 Dec 21. Int J Colorectal Dis. 2020. PMID: 31865435
References
-
- Williams NS, Marzouk DEMM, Hallan RI, et al. Function after ileal pouch and stapled pouch-anal anastomosis for ulcerative colitis. Br J Surg 1989; 76: 1168–1171. - PubMed
-
- Marcello PW, Roberts PL, Schoetz DJ, et al. Long-term results of the ileoanal pouch procedure. Arch Surg 1993; 128: 500–504. - PubMed
-
- Järvinen HJ, Luukkonen P. Experience with restorative proctocolectomy in 201 patients. Ann Chir Gynaecol 1993; 82: 159–164. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
