

Laryngeal recurrent nerve injury in surgery for benign thyroid diseases: effect of nerve dissection and impact of individual surgeon in more than 27,000 nerves at risk
- PMID: 11807367
- PMCID: PMC1422423
- DOI: 10.1097/00000658-200202000-00015
Laryngeal recurrent nerve injury in surgery for benign thyroid diseases: effect of nerve dissection and impact of individual surgeon in more than 27,000 nerves at risk
Abstract
Objective: To evaluate the effect of recurrent nerve dissection on the incidence of recurrent laryngeal nerve injury (RLNI) and to analyze the performance of individual surgeons.
Summary background data: Dissection of the recurrent nerve is mandatory in total thyroidectomy, but its relative merit in less extensive resections is not clear. The reported rates of RLNI differ widely; this may reflect a variation in the performance of individual surgeons.
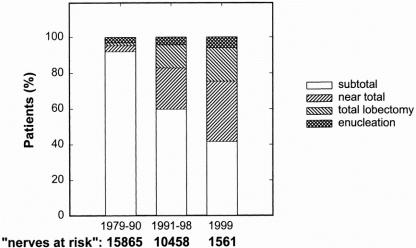
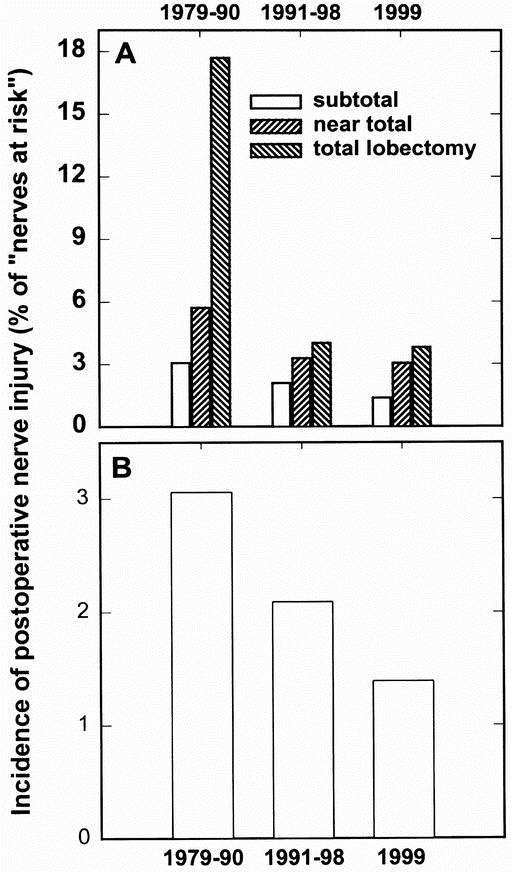
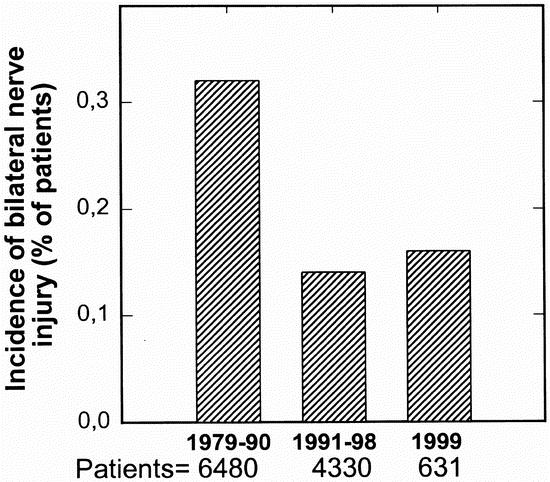
Methods: The authors studied the incidence of RLNI in primary surgery for benign thyroid disease during three periods in a single center. In period 1 (1979-1990; 9,385 consecutive patients, 15,865 nerves at risk), the recurrent nerve was not exposed. In period 2 (1991-1998; 6,128 patients, 10,548 nerves at risk), dissection of the recurrent nerve was the standard procedure. Global outcome and individual performance in these two periods were compared and presented to the surgeons. The effect of this quality control procedure was tested in 1999 (period 3; 930 patients, 1,561 nerves at risk).
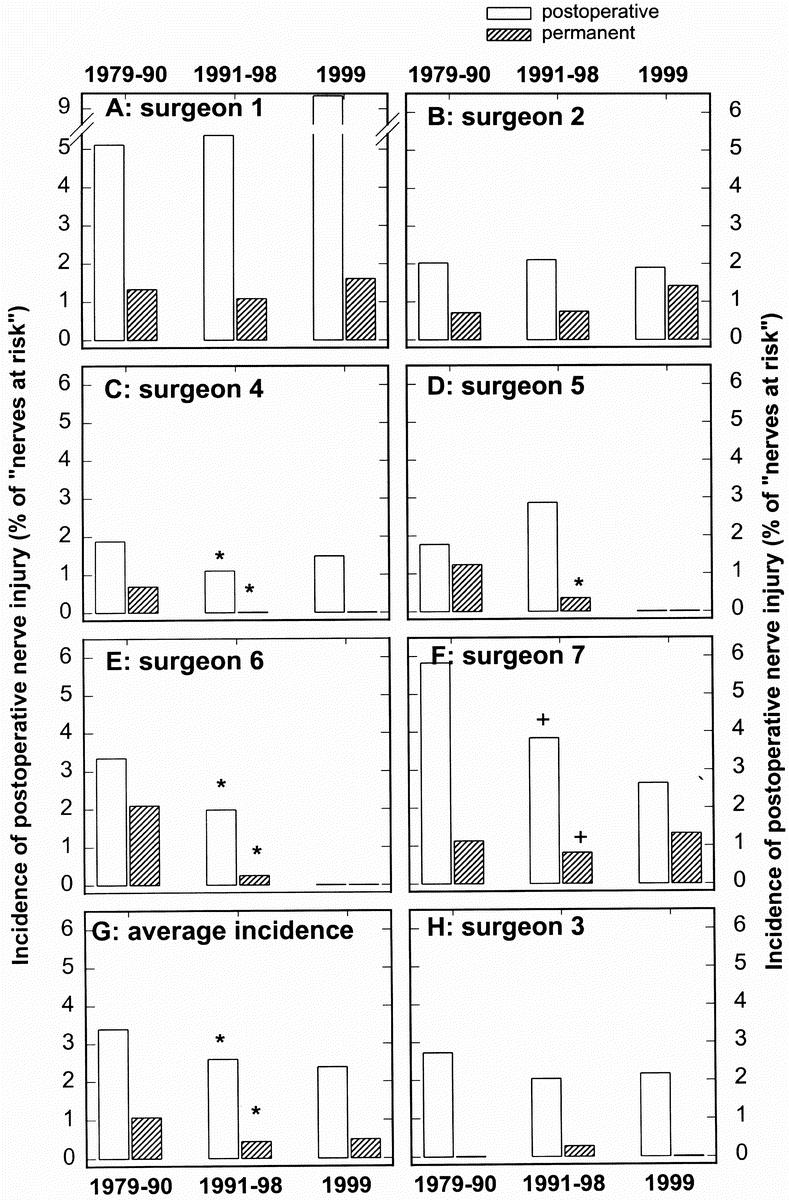
Results: Exposure of the recurrent nerve significantly reduced the global rate of postoperative and permanent RLNI. Some but not all surgeons improved their results by recurrent nerve dissection (e.g., permanent RLNI rates ranged from 0% to 1.1%). The documented significant differences in individual performances did not affect the outcome in period 3. The extent of nerve dissection was a source of variability; the rate of permanent RLNI averaged 0.9%, 0.3%, and 0.1% for surgeons who only localized, partially exposed, and completely dissected the recurrent nerve, respectively.
Conclusions: Recurrent nerve dissection significantly reduces the risk of RLNI. Extensive dissection facilitates visual control of nerve integrity during resection and is therefore superior to a more limited exposure of the nerve. Quality control can improve the global outcome and identify the variability in individual performance. This cannot be eliminated by merely confronting surgeons with comparative data; hence, it is important to search for the underlying causes.
Figures
References
-
- Blumenthal D. Part 1. Quality of care: what is it? N Engl J Med 1996; 335: 891–894. - PubMed
-
- Holli K, Laippala P, Ojala A, et al. Quality control in health care: an experiment in radiotherapy planning for breast cancer patients after mastectomy. Intl J Radiat Oncol Biol Phys 1999; 44: 827–833. - PubMed
-
- Ayanian JZ, Landrum MB, Normad SL, et al. Rating the appropriateness of coronary angiography: do practicing physicians agree with an expert panel and with each other? N Engl J Med 1998; 338: 1896–1904. - PubMed
-
- Schnelle JF, Cruis PA, Rahman A, et al. Developing rehabilitative behavioral interventions for long-term care: technology transfer, acceptance, and maintenance issues. J Am Geriatr Soc 1998; 46: 771–777. - PubMed
-
- Russel NS, Bartelink H. Radiotherapy: the last 25 years. Cancer Treatment Rev 1999; 25: 365–367. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
