

Use of magnetic resonance angiography to select candidates with recently symptomatic carotid stenosis for surgery: systematic review
- PMID: 11809640
- PMCID: PMC64789
- DOI: 10.1136/bmj.324.7331.198
Use of magnetic resonance angiography to select candidates with recently symptomatic carotid stenosis for surgery: systematic review
Abstract
Objective: To determine if sufficient evidence exists to support the use of magnetic resonance angiography as a means of selecting patients with recently symptomatic high grade carotid stenosis for surgery.
Design: Systematic review of published research on the diagnostic performance of magnetic resonance angiography, 1990-9.
Main outcome measures: Performance characteristics of diagnostic test.
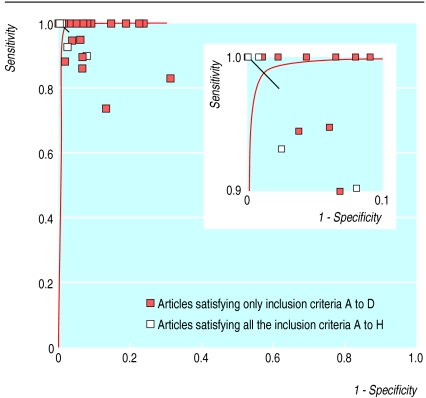
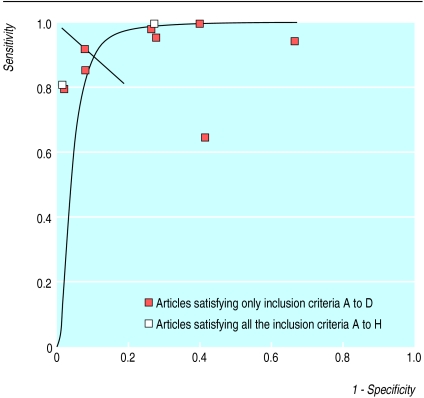
Results: 126 potentially relevant articles were identified, but many articles failed to examine the performance of magnetic resonance angiography as a diagnostic test at the surgical decision thresholds used in major clinical trials on endarterectomy. 26 articles were included in a meta-analysis that showed a maximal joint sensitivity and specificity of 99% (95% confidence interval 98% to 100%) for identifying 70-99% stenosis and 90% (81% to 99%) for identifying 50-99% stenosis. Only four articles evaluated contrast enhanced magnetic resonance angiography.
Conclusions: Magnetic resonance angiography is accurate for selecting patients for carotid endarterectomy at the surgical decision thresholds established in the major endarterectomy trials, but the evidence is not very robust because of the heterogeneity of the studies included. Research is needed to determine the diagnostic performance of the most recent developments in magnetic resonance angiography, including contrast enhanced techniques, as well as to assess the impact of magnetic resonance angiography on surgical decision making and outcomes.
Figures
Comment in
-
Review: magnetic resonance angiography is accurate for detecting high-grade carotid artery stenosis that is suitable for surgery.ACP J Club. 2002 Nov-Dec;137(3):110. ACP J Club. 2002. PMID: 12418850 No abstract available.
Similar articles
-
Duplex ultrasound for diagnosing symptomatic carotid stenosis in the extracranial segments.Cochrane Database Syst Rev. 2022 Jul 11;7(7):CD013172. doi: 10.1002/14651858.CD013172.pub2. Cochrane Database Syst Rev. 2022. PMID: 35815652 Free PMC article.
-
Accurate, practical and cost-effective assessment of carotid stenosis in the UK.Health Technol Assess. 2006 Aug;10(30):iii-iv, ix-x, 1-182. doi: 10.3310/hta10300. Health Technol Assess. 2006. PMID: 16904049
-
Duplex ultrasound and magnetic resonance angiography compared with digital subtraction angiography in carotid artery stenosis: a systematic review.Stroke. 2003 May;34(5):1324-32. doi: 10.1161/01.STR.0000068367.08991.A2. Epub 2003 Apr 10. Stroke. 2003. PMID: 12690221
-
Magnetic resonance perfusion for differentiating low-grade from high-grade gliomas at first presentation.Cochrane Database Syst Rev. 2018 Jan 22;1(1):CD011551. doi: 10.1002/14651858.CD011551.pub2. Cochrane Database Syst Rev. 2018. PMID: 29357120 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
Cited by
-
Prospective evaluation of carotid artery stenosis: elliptic centric contrast-enhanced MR angiography and spiral CT angiography compared with digital subtraction angiography.AJNR Am J Neuroradiol. 2003 May;24(5):1012-9. AJNR Am J Neuroradiol. 2003. PMID: 12748115 Free PMC article.
-
Imaging of carotid artery disease: from luminology to function?Neuroradiology. 2003 Oct;45(10):671-80. doi: 10.1007/s00234-003-1054-5. Epub 2003 Sep 4. Neuroradiology. 2003. PMID: 14564428 Review.
-
Time-of-flight MR angiography of carotid artery stenosis: does a flow void represent severe stenosis?AJNR Am J Neuroradiol. 2002 Nov-Dec;23(10):1779-84. AJNR Am J Neuroradiol. 2002. PMID: 12427639 Free PMC article.
-
Disappeared pulsatile tinnitus related to petrous segment stenosis of the ICA after relief of the stenosis by stenting.Interv Neuroradiol. 2013 Mar;19(1):97-101. doi: 10.1177/159101991301900115. Epub 2013 Mar 4. Interv Neuroradiol. 2013. PMID: 23472731 Free PMC article.
-
Evidence of bias and variation in diagnostic accuracy studies.CMAJ. 2006 Feb 14;174(4):469-76. doi: 10.1503/cmaj.050090. CMAJ. 2006. PMID: 16477057 Free PMC article.
References
-
- Edelman RR. MR angiography: present and future. Am J Roentgenol. 1993;161:1–11. - PubMed
-
- Erdoes LS, Marek JM, Mills JL, Berman SS, Whitehill T, Hunter GC, et al. The relative contributions of carotid duplex scanning, magnetic resonance angiography, and cerebral arteriography to clinical decisionmaking: a prospective study in patients with carotid occlusive disease. J Vasc Surg. 1996;23:950–956. - PubMed
-
- Barnett HJ, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes RB, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. N Engl J Med. 1998;339:1415–1425. - PubMed
-
- Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European carotid surgery trial (ECST) Lancet. 1998;351:1379–1387. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources