

Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement
- PMID: 11810682
- PMCID: PMC2041905
- DOI: 10.1002/mrm.10051
Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement
Abstract
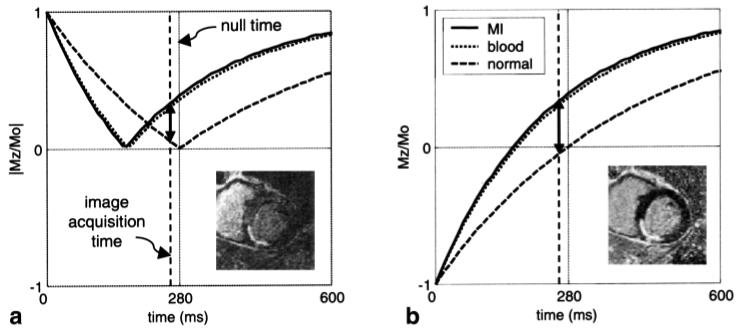
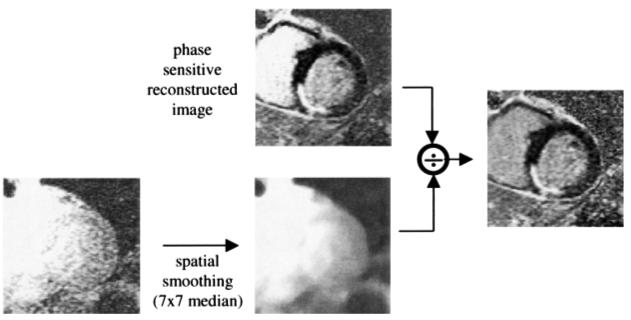
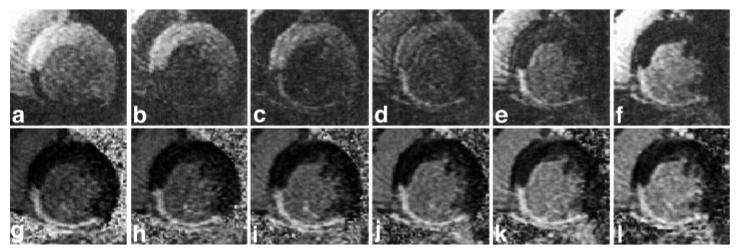
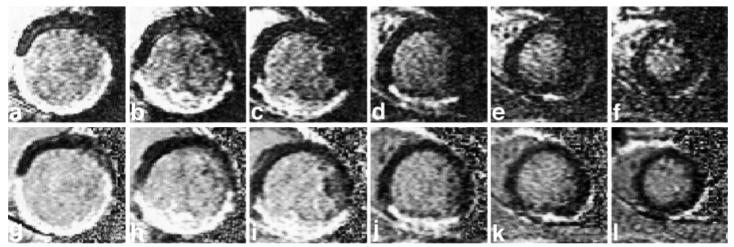
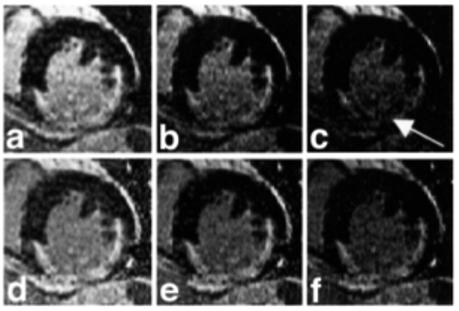
After administration of gadolinium, infarcted myocardium exhibits delayed hyperenhancement and can be imaged using an inversion recovery (IR) sequence. The performance of such a method when using magnitude-reconstructed images is highly sensitive to the inversion recovery time (TI) selected. Using phase-sensitive reconstruction, it is possible to use a nominal value of TI, eliminate several breath-holds otherwise needed to find the precise null time for normal myocardium, and achieve a consistent contrast. Phase-sensitive detection is used to remove the background phase while preserving the sign of the desired magnetization during IR. Experimental results are presented which demonstrate the benefits of both phase-sensitive IR image reconstruction and surface coil intensity normalization for detecting myocardial infarction (MI). The phase-sensitive reconstruction method reduces the variation in apparent infarct size that is observed in the magnitude images as TI is changed. Phase-sensitive detection also has the advantage of decreasing the sensitivity to changes in tissue T(1) with increasing delay from contrast agent injection.
Figures
References
-
- Kim RJ, Fieno DS, Parrish TB, Harris K, Chen EL, Simonetti O, Bundy J, Finn JP, Klocke FJ, Judd RM. Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation. 1999;100:1992–2002. - PubMed
-
- Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, Klocke FJ, Bonow RO, Judd RM. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343:1445–1453. - PubMed
-
- Kim RJ, Hillenbrand HB, Judd RM. Evaluation of myocardial viability by MRI. Herz. 2000;25:417–430. - PubMed
-
- Wu KC, Rochitte CE, Lima JA. Magnetic resonance imaging in acute myocardial infarction. Curr Opin Cardiol. 1999;14:480–484. - PubMed
-
- Simonetti OP, Kim RJ, Fieno DS, Hillenbrand HB, Wu E, Bundy JM, Finn JP, Judd RM. An improved MR imaging technique for the visualization of myocardial infarction. Radiology. 2001;218:215–223. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
