

A pilot randomised controlled trial of peripheral fractional oxygen extraction to guide blood transfusions in preterm infants
- PMID: 11815543
- PMCID: PMC1721368
- DOI: 10.1136/fn.86.1.f22
A pilot randomised controlled trial of peripheral fractional oxygen extraction to guide blood transfusions in preterm infants
Abstract
Background: Peripheral fractional oxygen extraction (FOE) may be a better indicator of the need for transfusion than the haemoglobin concentration (Hb) because it is a measure of the adequacy of oxygen delivery to meet demand. A randomised controlled trial of the use of peripheral FOE to guide the need for blood transfusions in preterm infants was carried out to test this hypothesis.
Method: Infants less than 1500 g birth weight who were stable and less than 2 weeks old were randomised to receive transfusions guided by either a conventional protocol based on Hb (conventional group) or a protocol based on measurements of peripheral FOE made by near infrared spectroscopy (NIRS group). Measurements of Hb and FOE were made on all infants from randomisation until discharge. The primary outcome measures were number of transfusions received, rate of weight gain, and postmenstrual age at discharge.
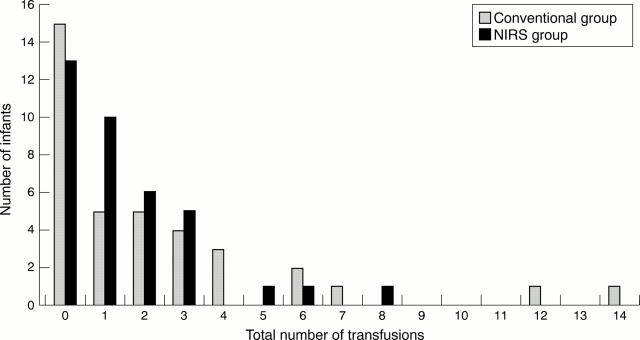
Results: Thirty seven infants were randomised to each group. Birth weight (median, range) (1200, 1004-1373 v 1136, 1009-1285 g) and Hb (median, range) at randomisation (160, 149-179 v 155, 145-181 g/l) did not differ between the two groups. The total number of transfusions given to the NIRS group was 56 and to the conventional group 84. The median number of transfusions per infant, the median volume of blood transfused to each group, and the total number of donors to which infants were exposed were similar in the two groups. Infants transfused according to the conventional protocol were more likely to be transfused earlier and at a higher Hb than those transfused in the NIRS group. Infants in the conventional group spent a significantly shorter period than those in the NIRS group with Hb < 100 g/l. Of the 56 transfusions given to the NIRS group, 33 (59%) were given because of clinical concerns rather than because of high FOE. There was no difference in the rate of weight gain, rate of linear growth, postmenstrual age at discharge, or the incidence of chronic lung disease or retinopathy of prematurity.
Conclusions: FOE measurements failed to identify many infants felt by clinicians to require blood transfusion. This may have been because clinicians relied on conventional indicators of transfusion that are vague and non-specific, or a peripheral FOE of 0.47 alone may not be a sensitive enough predictor of the need for transfusion. This requires further study.
Figures
Comment in
-
Blood transfusion in preterm neonates.Arch Dis Child Fetal Neonatal Ed. 2003 Jan;88(1):F78. doi: 10.1136/fn.88.1.f78. Arch Dis Child Fetal Neonatal Ed. 2003. PMID: 12496237 Free PMC article. No abstract available.
Similar articles
-
Peripheral fractional oxygen extraction and other measures of tissue oxygenation to guide blood transfusions in preterm infants.Semin Perinatol. 2001 Apr;25(2):60-4. doi: 10.1053/sper.2001.23200. Semin Perinatol. 2001. PMID: 11339666 Review.
-
Do cardiac output and serum lactate levels indicate blood transfusion requirements in anemia of prematurity?Intensive Care Med. 1996 May;22(5):472-6. doi: 10.1007/BF01712170. Intensive Care Med. 1996. PMID: 8796405
-
Splanchnic-cerebral oxygenation ratio as a marker of preterm infant blood transfusion needs.Transfusion. 2012 Feb;52(2):252-60. doi: 10.1111/j.1537-2995.2011.03263.x. Epub 2011 Jul 25. Transfusion. 2012. PMID: 21790634 Clinical Trial.
-
Differences in Cerebral Tissue Oxygenation in Preterm Neonates Receiving Adult or Cord Blood Red Blood Cell Transfusions.JAMA Netw Open. 2023 Nov 1;6(11):e2341643. doi: 10.1001/jamanetworkopen.2023.41643. JAMA Netw Open. 2023. PMID: 37934499 Free PMC article. Clinical Trial.
-
The near-infrared spectroscopy to evaluate neonatal improvement after transfusion: a systematic review and meta-analysis.BMC Pediatr. 2025 May 15;25(1):385. doi: 10.1186/s12887-025-05731-4. BMC Pediatr. 2025. PMID: 40375204 Free PMC article.
Cited by
-
Functional echocardiographic assessment of myocardial performance in anemic premature infants: a pilot study.Pediatr Cardiol. 2012 Apr;33(4):554-61. doi: 10.1007/s00246-012-0154-6. Epub 2012 Jan 25. Pediatr Cardiol. 2012. PMID: 22274640
-
Red Blood Cell Transfusion Thresholds for Anemia of Prematurity.Neoreviews. 2023 Jun 1;24(6):e370-e376. doi: 10.1542/neo.24-6-e370. Neoreviews. 2023. PMID: 37258497 Free PMC article. Review.
-
When to transfuse preterm babies.Arch Dis Child Fetal Neonatal Ed. 2008 Nov;93(6):F469-73. doi: 10.1136/adc.2007.128819. Epub 2008 Jul 24. Arch Dis Child Fetal Neonatal Ed. 2008. PMID: 18653585 Free PMC article. Review.
-
Regional tissue oxygenation and conventional indicators of red blood cell transfusion in anaemic preterm infants.EClinicalMedicine. 2022 Apr 4;46:101365. doi: 10.1016/j.eclinm.2022.101365. eCollection 2022 Apr. EClinicalMedicine. 2022. PMID: 35399813 Free PMC article.
-
The light still shines, but not that brightly? The current status of perinatal near infrared spectroscopy.Arch Dis Child Fetal Neonatal Ed. 2003 Jul;88(4):F263-8. doi: 10.1136/fn.88.4.f263. Arch Dis Child Fetal Neonatal Ed. 2003. PMID: 12819155 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical