

Clinical characteristics and outcome of a cohort of 101 patients with hepatocellular carcinoma
- PMID: 11819762
- PMCID: PMC4723524
- DOI: 10.3748/wjg.v7.i2.208
Clinical characteristics and outcome of a cohort of 101 patients with hepatocellular carcinoma
Abstract
Aim: To conduct a cohort study of 101 patients with hepatocellular carcinoma (HCC) presenting to a tertiary care medical referral center in Germany between 1997 and 1999.
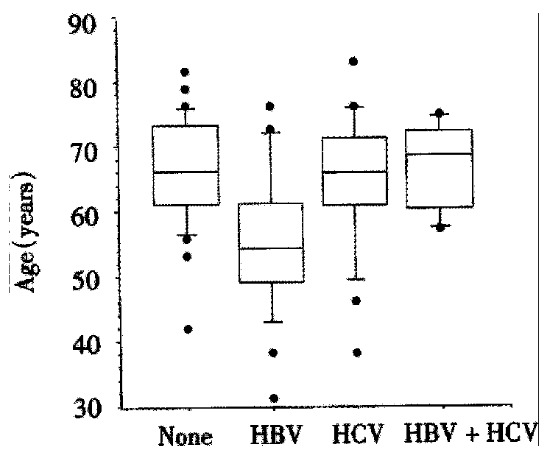
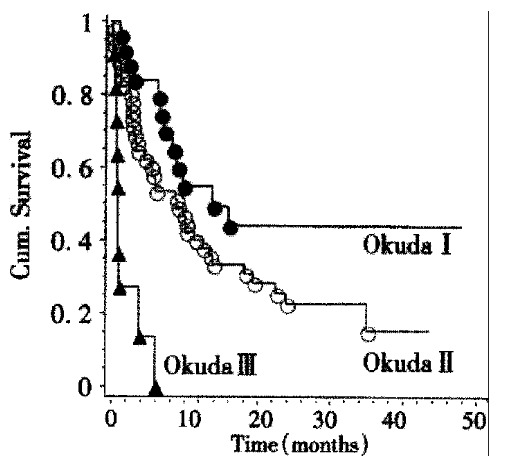
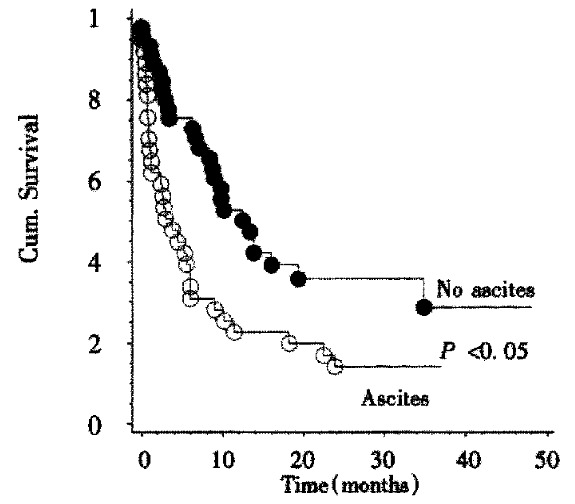
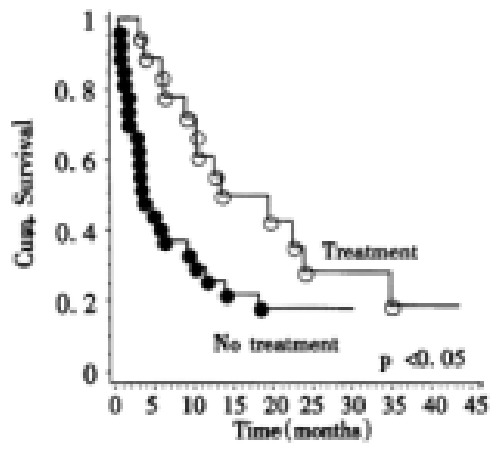
Methods and results: Data were retrospectively analyzed by chart review. In 95 cases (72 males and 23 females) sufficient data were available for analysis. Twenty five (29%) of 85 patients were HBsAg or anti HBc positive, 21/85 (25%) were anti HCV positive, and 6/85 (7%) were positive for both HBV and HCV-markers. Age was significantly lower in HBV positive patients than in the other two groups. Thirty one (34%) of 90 patients had histories of alcohol abuse. In 79/94 (84%) patients, cirrhosis was diagnosed. Of these cirrhotic patients, 29/79 (37%) belonged to Child Pugh's group (CHILD) A, 32/79 (40%) to CHILD B, and 18/79 (23%) to CHILD C. AFP was elevated in 61/91 (67%) patients. A single tumor nodule was found in 38/94 (40%), more than one nodule in 31/94 (34%), and 25/94 (26%) had a diffusely infiltrating tumor, i.e. the tumor margins could not be seen on imaging procedures. Portal vein thrombosis was present in 19/94 (20%). Imaging data consistent with lymph node metastases were found in 10/92 (11%), while distant metastases were found in 8/93 (9%). According to Okuda 28/94 (30%) were grouped to stage I, 53/94 (56%) were grouped to stage II, and 13/94 (14%) were grouped to stage II. Survival data were available for 83 patients. The Kaplan-Meier estimate for median survival was 8 4 months. Factors influencing survival were the Okuda score, the presence of portal vein thrombosis, and the presence of ascites. The presence of non complicated liver cirrhosis by itself, distant metastases, or infection with hepatitis viruses did not influence survival. AFP positivity by itself did not influence survival, though patients with an AFP value greater than 100 microg/L did experience shortened survival. Treatment besides tamoxifen or supportive care was associated with prolonged survival. The influence of therapy on survival was most pronounced in Okuda stage II patients. There was longer survival in those Okuda stage II patients who were treated with percutaneous ethanol injection.
Conclusion: Even in a low incidence area such as Germany, the majority of HCC is caused by viral hepatitis and therefore potentially preventable. Reflecting the high proportion of advanced stage tumors in our patients, the median survival was poor. Patients who received active therapy had a longer survival.
Figures
References
-
- WHO. World Health Report. Geneva: WHO; 2000.
-
- Blakely T, Bates M, Garrett N, Robson B. The incidence of hepatocellular carcinoma in New Zealand. N Z Med J. 1998;111:471–474. - PubMed
-
- Blakely TA, Bates MN, Baker MG, Tobias M. Hepatitis B carriage explains the excess rate of hepatocellular carcinoma for Maori, Pacific Island and Asian people compared to Europeans in New Zealand. Int J Epidemiol. 1999;28:204–210. - PubMed
-
- Beasley RP, Hwang LY, Lin CC, Chien CS. Hepatocellular carcinoma and hepatitis B virus. A prospective study of 22 707 men in Taiwan. Lancet. 1981;2:1129–1133. - PubMed
-
- Beasley RP. Hepatitis B virus. The major etiology of hepatocellular carcinoma. Cancer. 1988;61:1942–1956. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
