

Combined clinical and imaging information as an early stroke outcome measure
- PMID: 11823654
- PMCID: PMC2749233
- DOI: 10.1161/hs0202.102881
Combined clinical and imaging information as an early stroke outcome measure
Abstract
Background and purpose: Imaging information has been proposed as a potential surrogate outcome in stroke clinical trials. The purpose of this study was to determine whether an early outcome measure combining clinical and imaging information is better than either alone in predicting 3-month outcome in acute ischemic stroke patients.
Methods: Clinical information (National Institutes of Health Stroke Scale) and imaging information (CT infarct volume), measured at 1 week from 201 patients from the Randomized Trial of Tirilazad Mesylate in Acute Stroke (RANTTAS) study, were used in a multivariable logistic regression analysis to predict excellent and devastating 3-month outcome. The combined models were compared with the infarct volume models and the clinical models. Discrimination, calibration, and change in global model chi-square were assessed.
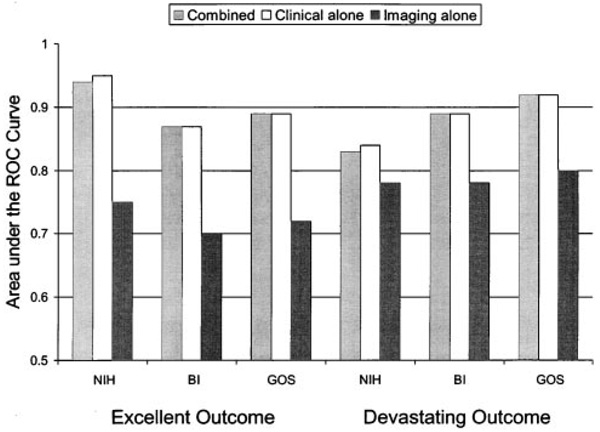
Results: The combined models and models using clinical information alone had areas under the receiver operating characteristic curves that did not differ significantly (probability value = 0.092 to 0.4), ranging from 0.83 to 0.95. The imaging alone models performed less well (P<0.005) and had areas under the receiver operating characteristic curves that ranged from 0.70 to 0.80.
Conclusions: The National Institutes of Health Stroke Scale at 1 week is highly predictive of 3-month outcome in ischemic stroke patients. The addition of 1-week infarct volume does not improve the accuracy of the predictive model.
Figures
References
-
- Warach S, Pettigrew LC, Dashe JF, Pullicino P, Lefkowitz DM, Sabounjian L, Harnett K, Schwiderski U, Gammans R. Effect of citicoline on ischemic lesions as measured by diffusion-weighted magnetic resonance imaging. Citicoline 010 Investigators. Ann Neurol. 2000;48:713–722. - PubMed
-
- Warach S, Boska M, Welch KMA. Pitfalls and potential of clinical diffusion-weighted MR imaging in acute stroke. Stroke. 1997;28:481–482. - PubMed
-
- Lovblad KO, Baird AE, Schlaug G, Benfield A, Siewert B, Voetsch B, Connor A, Burzynski C, Edelman RR, Warach S. Ischemic lesion volumes in acute stroke by diffusion-weighted magnetic resonance imaging correlate with clinical outcome. Ann Neurol. 1997;42:164–170. - PubMed
-
- Warach S, Moseley M, Johnston K, Adams H, Zivin J. Diffusion weighted imaging: ready for prime time?. Plenary Session Presented at the 23rd International Joint Conference on Stroke and Cerebral Circulation; February 5; Orlando, Fla. 1998.
-
- Thijs BN, Lansberg MG, Beaulieu C, Marks MP, Moseley ME, Albers GW. Is early ischemic lesion volume on diffusion-weighted imaging an independent predictor of stroke outcome? A multivariable analysis. Stroke. 2000;31:2597–2602. - PubMed
