

Evaluation of use of Epstein-Barr viral load in patients after allogeneic stem cell transplantation to diagnose and monitor posttransplant lymphoproliferative disease
- PMID: 11825941
- PMCID: PMC153400
- DOI: 10.1128/JCM.40.2.351-358.2002
Evaluation of use of Epstein-Barr viral load in patients after allogeneic stem cell transplantation to diagnose and monitor posttransplant lymphoproliferative disease
Erratum in
- J Clin Microbiol 2002 Jun;40(6):2316
Abstract
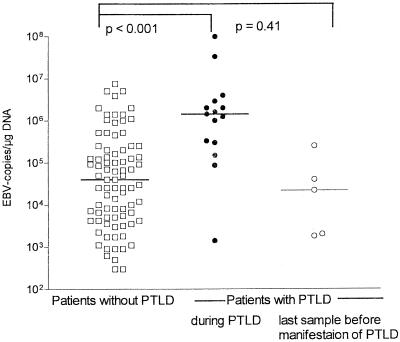
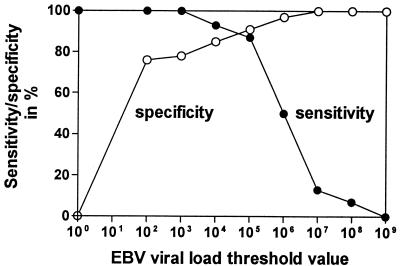
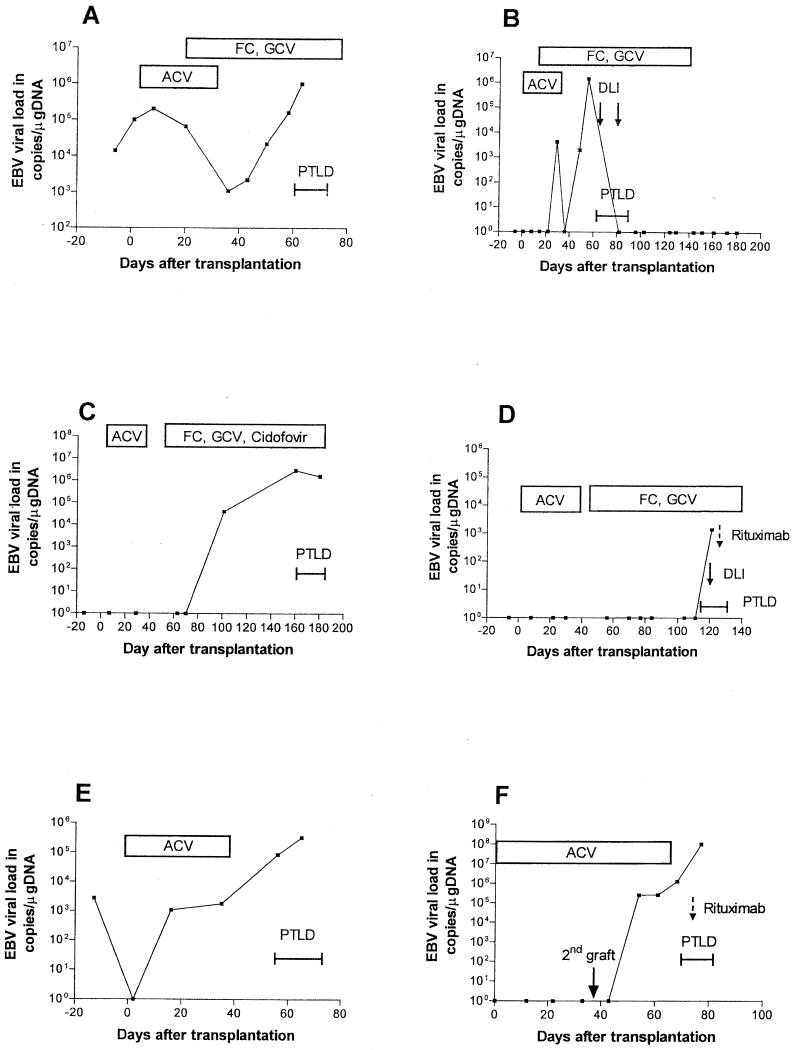
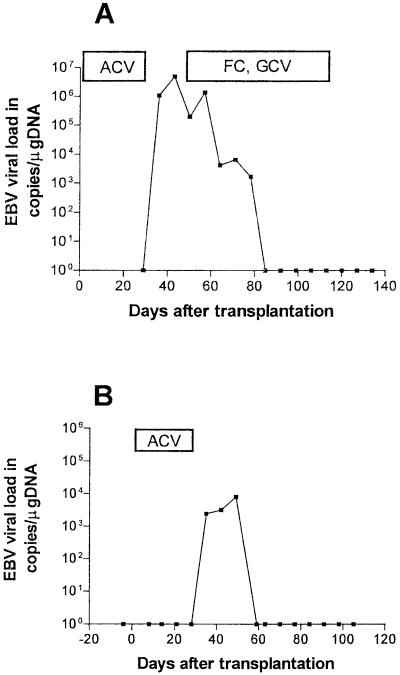
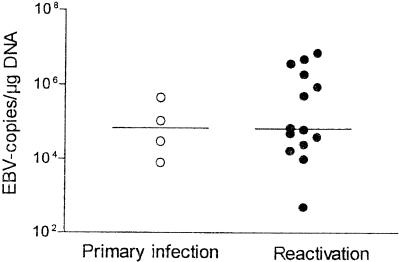
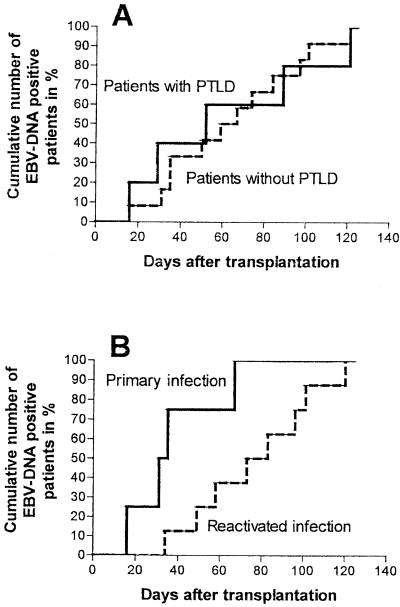
Epstein-Barr virus (EBV)-induced posttransplant lymphoproliferative disease (PTLD) continues to be a serious complication following transplantation. The aim of the present study was to evaluate the EBV load as a parameter for the prediction and monitoring of PTLD. The EBV load was analyzed by a quantitative competitive PCR with 417 whole-blood samples of 59 patients after allogeneic stem cell transplantation (SCT). The EBV load was positive for all 9 patients with PTLD and for 17 patients without PTLD. The viral loads of patients with manifest PTLD differed from the loads of those without PTLD (median loads, 1.4 x 10(6) versus 4 x 10(4) copies/microg of DNA; P < 0.0001). A threshold value of 10(5) copies/microg of DNA showed the best diagnostic efficacy (sensitivity, 87%; specificity, 91%). However, in patients with less than three major risk factors for PTLD, the positive predictive value of this threshold was rather low. One week prior to the manifestation of PTLD, the EBV load was as low in patients who developed PTLD as in patients without disease (median, 2.2 x 10(4) copies/microg of DNA; P was not significant). EBV DNA tested positive first at 20 to 71 days prior to the clinical manifestation of PTLD and occurred with the same delay after transplantation regardless of disease (median delay, 52 versus 63 days; P was not significant). EBV DNA was detected earlier in patients with primary infections than in those with reactivations (33 versus 79 days; P = 0.01), but the peak levels were similar in the two groups. EBV primary infection or EBV reactivation is frequent in patients after allogeneic SCT but results in PTLD only in a subgroup of patients. Although evaluation of the EBV load has limitations, the EBV load represents a valuable parameter to guide therapy.
Figures
References
-
- Baldanti, F., P. Grossi, M. Furione, L. Simoncini, A. Sarasini, P. Comoli, R. Maccario, R. Fiocchi, and G. Gerna. 2000. High levels of Epstein-Barr virus DNA in blood of solid-organ transplant recipients and their value in predicting posttransplant lymphoproliferative disorders. J. Clin. Microbiol. 38:613-619. - PMC - PubMed
-
- Craig, F. E., M. L. Gulley, and P. M. Banks. 1993. Posttransplantation lymphoproliferative disorders. Am. J. Clin. Pathol. 99:265-276. - PubMed
-
- Curtis, R. E., L. B. Travis, P. A. Rowlings, G. Socie, D. W. Kingma, P. M. Banks, E. S. Jaffe, G. E. Sale, M. M. Horowitz, R. P. Witherspoon, D. A. Shriner, D. J. Weisdorf, H. J. Kolb, K. M. Sullivan, K. A. Sobocinski, R. P. Gale, R. N. Hoover, J. F. Fraumeni, Jr., and H. J. Deeg. 1999. Risk of lymphoproliferative disorders after bone marrow transplantation: a multi-institutional study. Blood 94:2208-2216. - PubMed
-
- Darenkov, I. A., M. A. Marcarelli, G. P. Basadonna, A. L. Friedman, K. M. Lorber, J. G. Howe, J. Crouch, M. J. Bia, A. S. Kliger, and M. I. Lorber. 1997. Reduced incidence of Epstein-Barr virus-associated posttransplant lymphoproliferative disorder using preemptive antiviral therapy. Transplantation 64:848-852. - PubMed
-
- Einsele, H., G. Ehninger, H. Hebart, K. M. Wittkowski, U. Schuler, G. Jahn, P. Mackes, M. Herter, T. Klingebiel, J. Loffler, et al. 1995. Polymerase chain reaction monitoring reduces the incidence of cytomegalovirus disease and the duration and side effects of antiviral therapy after bone marrow transplantation. Blood 86:2815-2820. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
