

Variations in mortality rates among Canadian neonatal intensive care units
- PMID: 11826939
- PMCID: PMC99269
Variations in mortality rates among Canadian neonatal intensive care units
Abstract
Background: Most previous reports of variations in mortality rates for infants admitted to neonatal intensive care units (NICUs) have involved small groups of subpopulations, such as infants with very low birth weight. Our aim was to examine the incidence and causes of death and the risk-adjusted variation in mortality rates for a large group of infants of all birth weights admitted to Canadian NICUs.
Methods: We examined the deaths that occurred among all 19 265 infants admitted to 17 tertiary-level Canadian NICUs from January 1996 to October 1997. We used multivariate analysis to examine the risk factors associated with death and the variations in mortality rates, adjusting for risks in the baseline population, severity of illness on admission and whether the infant was outborn (born at a different hospital from the one where the NICU was located).
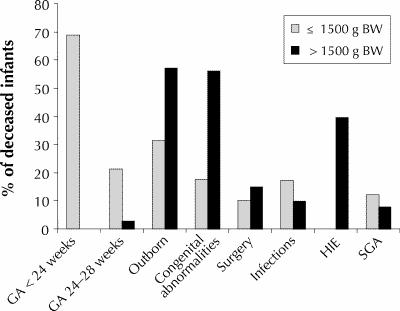
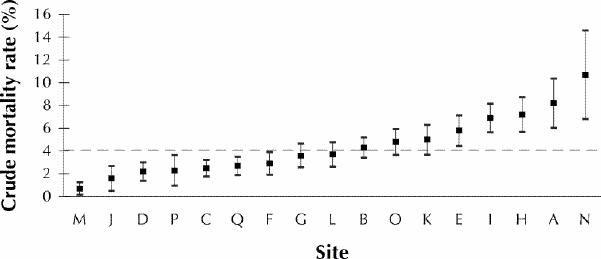
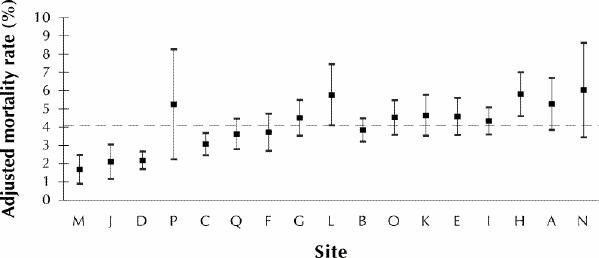
Results: The overall mortality rate was 4% (795 infants died). Forty percent of the deaths (n = 318) occurred within 2 days of NICU admission, 50% (n = 397) within 3 days and 75% (n = 596) within 12 days. The major conditions associated with death were gestational age less than 24 weeks (59 deaths [7%]), gestational age 24-28 weeks (325 deaths [41%]), outborn status (340 deaths [42%]), congenital anomalies (270 deaths [34%]), surgery (141 deaths [18%]), infection (108 deaths 114%]), hypoxic-ischemic encephalopathy (128 deaths [16%]) and small for gestational age (i.e., less than the third percentile) (77 deaths [10%]). There was significant variation in the risk-adjusted mortality rates (range 1.6% to 5.5%) among the 17 NICUs.
Interpretation: Most NICU deaths occurred within the first few days after admission. Preterm birth, outborn status and congenital anomalies were the conditions most frequently associated with death in the NICU. The significant variation in risk-adjusted mortality rates emphasizes the importance of risk adjustment for valid comparison of NICU outcomes.
Figures
Comment in
-
Variations in mortality rates among Canadian neonatal intensive care units: interpretation and implications.CMAJ. 2002 Jan 22;166(2):191-2. CMAJ. 2002. PMID: 11826942 Free PMC article. No abstract available.
-
What's in a name? Reporting data from public institutions.CMAJ. 2002 Jan 22;166(2):193-4. CMAJ. 2002. PMID: 11826943 Free PMC article. No abstract available.
-
Variations in mortality rates among Canadian NICUs--and anonymous reporting.CMAJ. 2002 Jul 23;167(2):120; author reply 120-1. CMAJ. 2002. PMID: 12160111 Free PMC article. No abstract available.
Similar articles
-
First year mortality and hospital morbidity after newborn intensive care.N Z Med J. 1987 Sep 9;100(831):548-52. N Z Med J. 1987. PMID: 3451137
-
Variations in rates of nosocomial infection among Canadian neonatal intensive care units may be practice-related.BMC Pediatr. 2005 Jul 8;5:22. doi: 10.1186/1471-2431-5-22. BMC Pediatr. 2005. PMID: 16004613 Free PMC article.
-
Improved outcomes of outborn preterm infants if admitted to perinatal centers versus freestanding pediatric hospitals.J Pediatr. 2005 May;146(5):626-31. doi: 10.1016/j.jpeds.2005.01.030. J Pediatr. 2005. PMID: 15870665
-
Infant mortality statistics from the 2004 period linked birth/infant death data set.Natl Vital Stat Rep. 2007 May 2;55(14):1-32. Natl Vital Stat Rep. 2007. PMID: 17569269 Review.
-
Risk adjustment for quality improvement.Pediatrics. 1999 Jan;103(1 Suppl E):255-65. Pediatrics. 1999. PMID: 9917469 Review.
Cited by
-
Admissions and mortality over a 5-year period in a limited-resource neonatal unit in Ghana.Ghana Med J. 2019 Jun;53(2):117-125. doi: 10.4314/gmj.v53i2.6. Ghana Med J. 2019. PMID: 31481807 Free PMC article.
-
What's in a name? Reporting data from public institutions.CMAJ. 2002 Jan 22;166(2):193-4. CMAJ. 2002. PMID: 11826943 Free PMC article. No abstract available.
-
Neonatal intensive care unit safety culture varies widely.Arch Dis Child Fetal Neonatal Ed. 2012 Mar;97(2):F120-6. doi: 10.1136/archdischild-2011-300635. Epub 2011 Sep 19. Arch Dis Child Fetal Neonatal Ed. 2012. PMID: 21930691 Free PMC article.
-
Systematic review and meta-analysis of clinical outcomes of early caffeine therapy in preterm neonates.Br J Clin Pharmacol. 2017 Jan;83(1):180-191. doi: 10.1111/bcp.13089. Epub 2016 Sep 30. Br J Clin Pharmacol. 2017. PMID: 27526255 Free PMC article.
-
The regionalization of pediatric health care.Pediatrics. 2010 Dec;126(6):1182-90. doi: 10.1542/peds.2010-1119. Epub 2010 Nov 1. Pediatrics. 2010. PMID: 21041285 Free PMC article. Review.
References
-
- Stahlman MT. Newborn intensive care: Success or failure? J Pediatr 1984; 105: 162-7. - PubMed
-
- Hack M, Wright LL, Shankaran S, Tyson JE, Horbar JD, Bauer CR, et al. Very low birth weight outcomes of the National Institute of Child Health and Human Development Neonatal Network, November 1989 to October 1990. Am J Obstet Gynecol 1995;172:457-64. - PubMed
-
- Horwood SP, Boyle MP, Torrance GW, Sinclair JC. Mortality and morbidity of 500 to 1,499 gram birth weight infants live-born to residents of a defined geographic region before and after neonatal intensive care. Pediatrics 1982; 69:613-20. - PubMed
-
- Williams RL, Chen PM. Identifying the sources of the recent decline in perinatal mortality rates in California. N Engl J Med 1982;306:207-14. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources