

Radial width of the temporal horn: a sensitive measure in Alzheimer disease
- PMID: 11827874
- PMCID: PMC7975508
Radial width of the temporal horn: a sensitive measure in Alzheimer disease
Abstract
Background and purpose: Atrophy in the medial temporal lobe (MTL) structures depicted with brain imaging is one of the most accurate markers of Alzheimer disease (AD), but practical considerations have thus far limited their routine clinical use. The aim of this study was to explore the validity of a CT- and MR-based measure of MTL atrophy that would be feasible for routine clinical use.
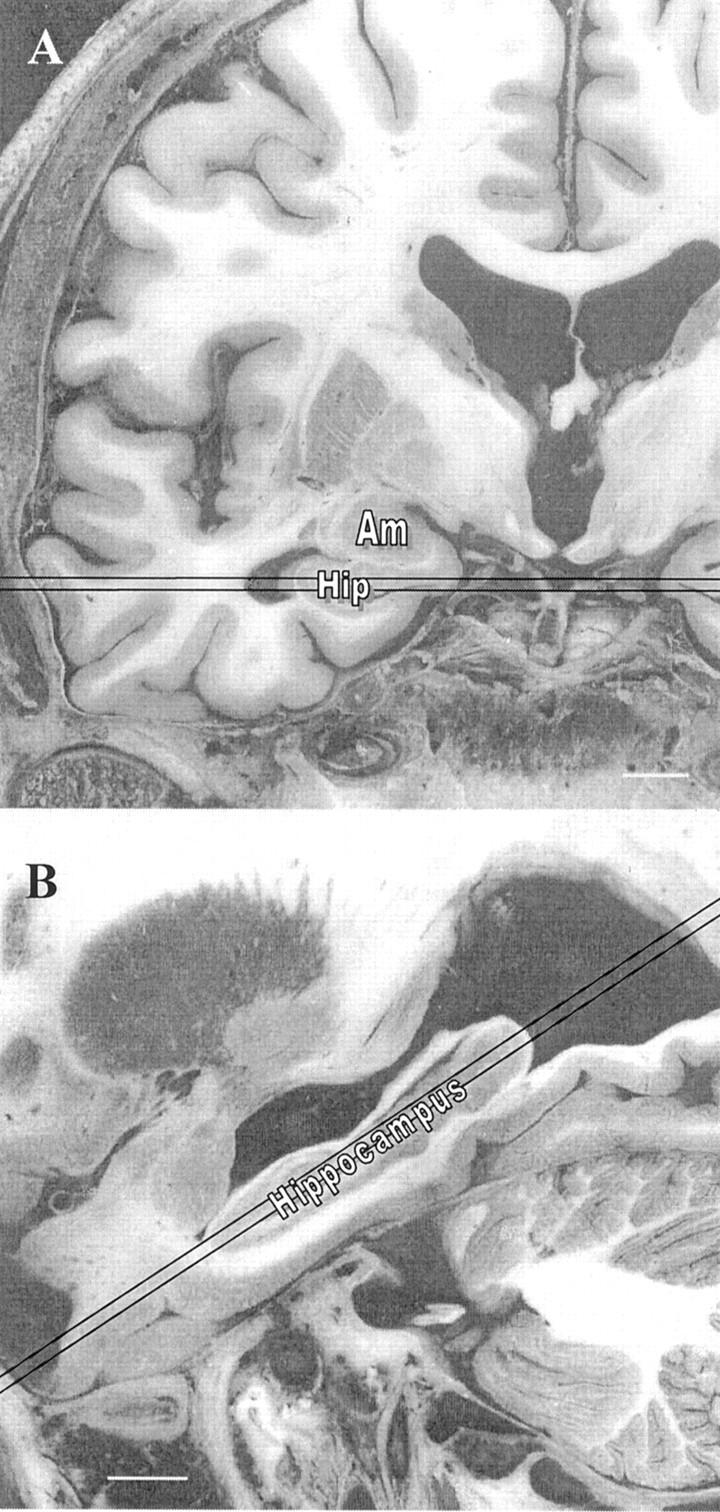
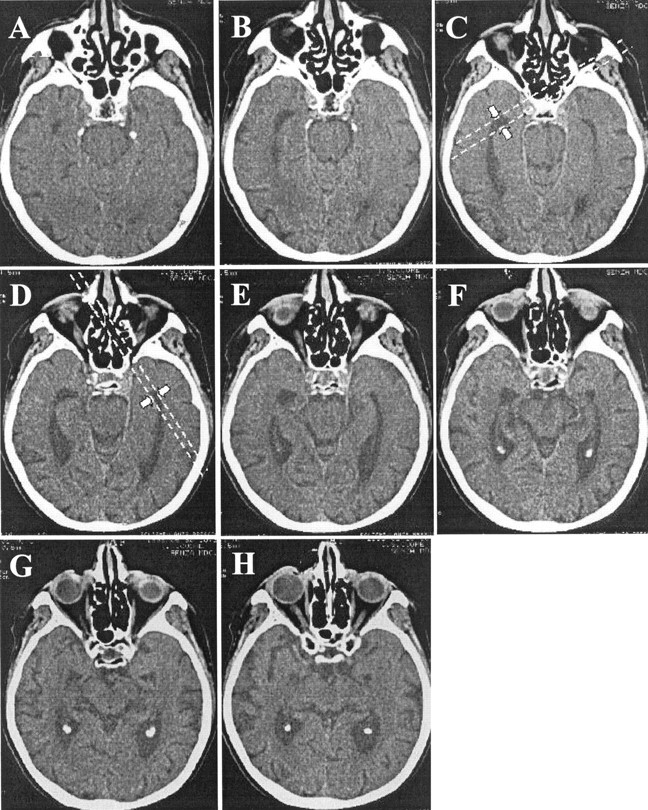
Methods: We acquired brain CT scans in the temporal lobe plane with thin sections in 42 patients with AD and in 29 control patients without dementia. We also acquired MR images (according to a 3D magnetization-prepared rapid gradient-echo protocol) in 28 patients with AD and in 28 control subjects without dementia. The radial width of the temporal horn (rWTH) of the lateral ventricle was measured with a precision caliper at the tip of the horn on CT scans or high-quality MR images. The validity of the rWTH variable was assessed by test-retest and interrater reliability, convergent and discriminant validity compared with progressively distant brain regions, and known-group validity (accuracy of the separation of patients with AD from control subjects). Convergent and discriminant validity compared with volumetric measures was tested in the patients who underwent MR imaging.
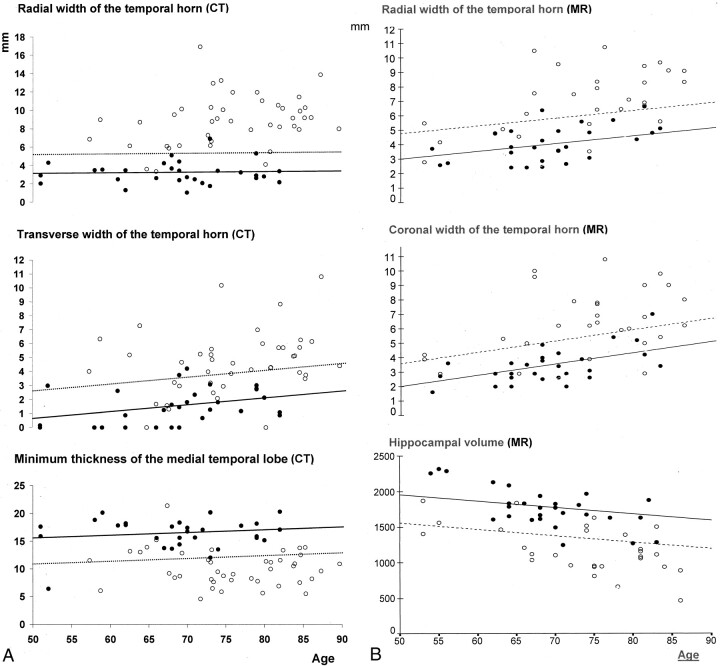
Results: Intraclass correlation coefficients for inter- and intrarater reliability were between 0.94 and 0.98. On CT scans, Pearson's correlation of the rWTH with the transverse width of the temporal horn was between 0.60 and 0.79; with Jobst's minimum thickness of the MTL, between 0.63 and 0.78 (interuncal distance approximately 0.50); and with an index of frontal atrophy, between 0.35 and 0.42. On MR images, the correlation with volumetric MR measures was 0.80 in the temporal horn, 0.74 in the hippocampus, 0.68 in the temporal lobe, 0.58 in the entorhinal cortex, and 0.49 in the frontal lobe. On CT scans (cutoff value for AD, >5.3 mm; age range of subjects, 50-90 y), the rWTH measure was a sensitive marker for AD in 39 of 42 patients with AD (sensitivity, 93%) and was a specific marker in 28 of the 29 control patients (specificity, 97%). On MR images (cutoff 3.6-6.7 mm; age range of subject, 50-90 y), the rWTH was a sensitive marker for AD in 21 of 28 patients with AD (sensitivity, 75%) and was a specific marker in 26 of 28 control subjects (specificity, 93%). The accuracy of other linear CT-based measures of MTL atrophy and linear and volumetric MR-based measures was lower. With specificity set to 95%, sensitivity ranged from 57% to 74% for CT-based measures and from 52% to 74% for MR-based measures.
Conclusion: The rWTH is an accurate marker of AD that could be used in routine clinical settings.
Figures
Comment in
-
The magic measurement.AJNR Am J Neuroradiol. 2004 Jan;25(1):158-9; author reply 159. AJNR Am J Neuroradiol. 2004. PMID: 14729549 Free PMC article. No abstract available.
References
-
- Radebaugh TS, Khachaturian S, eds. Report of the Working Group on Biological Markers of Alzheimer’s Disease. Chicago: Ronald and Nancy Reagan Research Institute–Alzheimer’s Association; 1997
-
- Juottonen K, Laakso MP, Partanen K, Soininen H. Comparative MRI analysis of the entorhinal cortex and hippocampus in diagnosing Alzheimer’s disease. AJNR Am J Neuroradiol 1999;20:139–144 - PubMed
-
- Laakso MP, Soininen H, Partanen K, et al. MRI of the hippocampus in Alzheimer’s disease: sensitivity, specificity, and analysis of the incorrectly classified subjects. Neurobiol Aging 1998;19:23–31 - PubMed
-
- DeCarli C, Kaye JA, Horwitz B, Rapoport SI. Critical analysis of the use of computer-assisted transverse axial tomography to study human brain in aging and dementia of the Alzheimer type. Neurology 1990;40:872–883 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical