

Prospective evaluation of suspected stenoocclusive disease of the intracranial artery: combined MR angiography and CT angiography compared with digital subtraction angiography
- PMID: 11827880
- PMCID: PMC7975497
Prospective evaluation of suspected stenoocclusive disease of the intracranial artery: combined MR angiography and CT angiography compared with digital subtraction angiography
Abstract
Background and purpose: MR angiography is primarily and increasingly used to assess intracranial arterial stenoocclusion. However, MR angiography can cause overestimation of stenosis. Although CT angiography is accurate, it has limitations. Our purpose was to determine whether the accuracy of combined MR angiography and CT angiography is equal to that of digital subtraction angiography (DSA) in measuring stenosis and detecting major intracranial arterial occlusion.
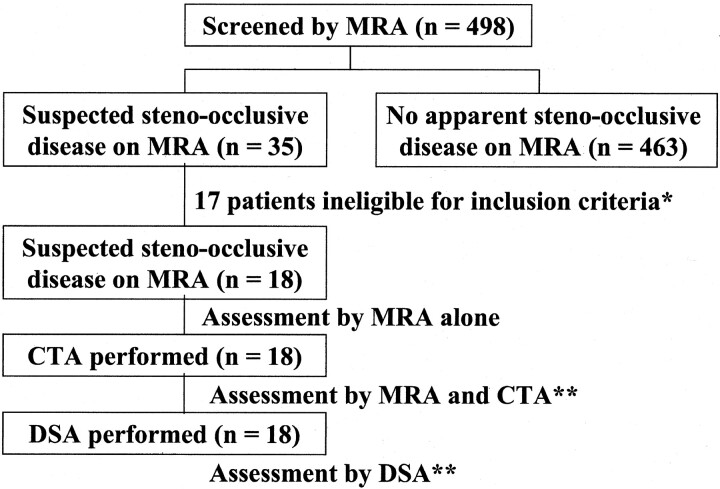
Methods: CT angiography and intraarterial DSA were prospectively performed in 18 patients with suspected intracranial stenoocclusive disease, as revealed with MR angiography. Before DSA, two reviewers independently assessed MR intracranial angiograms. Subsequently, they assessed CT angiograms with MR angiograms. Results were compared with DSA results. The degree of stenoocclusion was categorized; stenosis of 50% or more indicated stenoocclusive disease. After the blinded study, two radiologists retrospectively reviewed the angiographic findings.
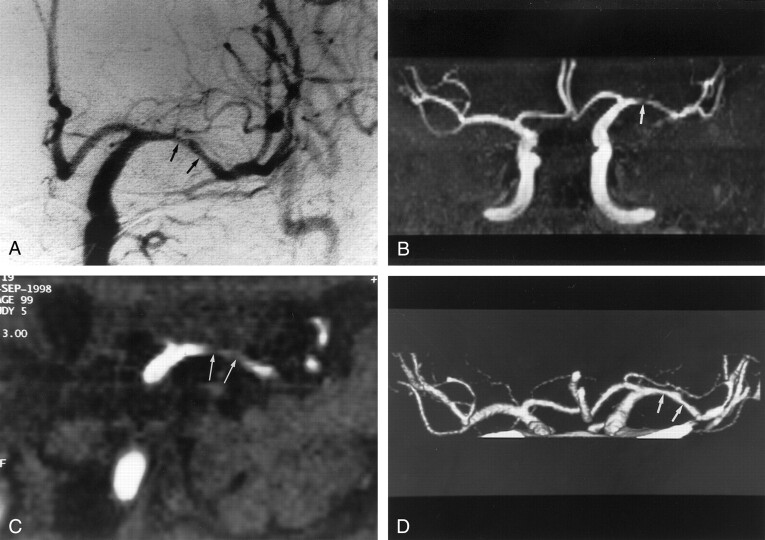
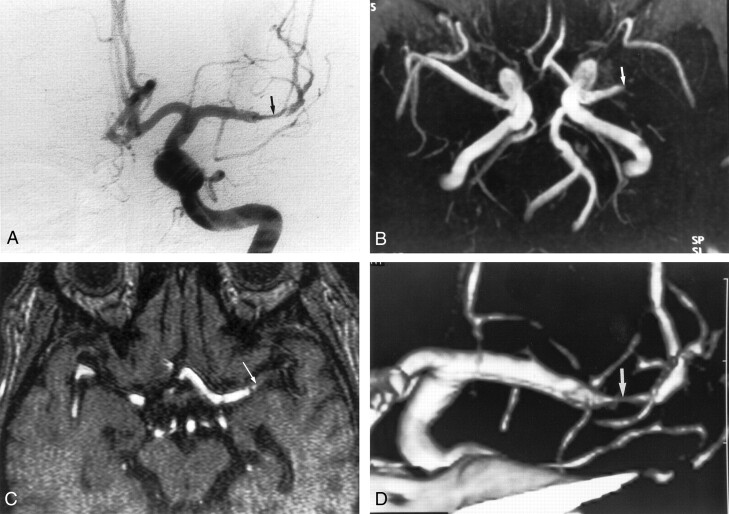
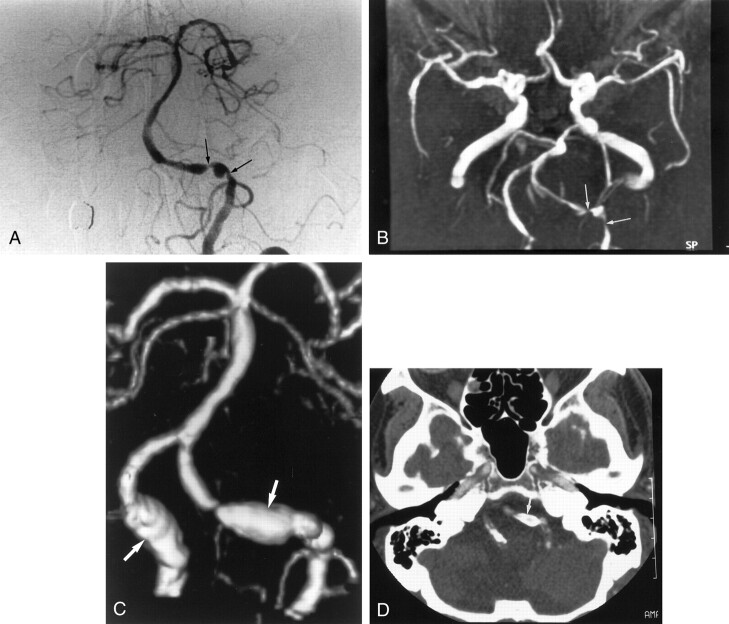
Results: Stenoocclusive disease was identified in 18 of 198 intracranial arteries at DSA. MR angiography had a sensitivity of 92%, a specificity of 91%, and an accuracy of 91% for the identification of stenosis of 50% or more; the addition of CT angiography yielded values of 100%, 99%, and 99%, respectively. Stenotic grades with combined CT angiography and MR angiography agreed with those of DSA in 98% of cases. In the retrospective study, CT angiography did not always correctly delineate arterial lumina with circumferential calcification and cavernous portions of the internal carotid artery.
Conclusion: In this investigation, the evaluation of suspected stenoocclusive diseases in major intracranial arteries, the accuracy of combined MR angiography and CT angiography is equal to that of DSA in most cases.
Figures
References
-
- Sacco RL, Kargman DE, Gu Q, Zamanillo MC. Race-ethnicity and determinants of intracranial atherosclerotic cerebral infarction: the Northern Manhattan Stroke Study. Stroke 1995;26:14–20 - PubMed
-
- Chimowitz MI, Kokkinos J, Strong J, et al. The Warfarin-Aspirin Symptomatic Intracranial Disease Study. Neurology 1995;45:1488–1493 - PubMed
-
- Heiserman JE, Drayer BP, Keller PJ, Fram EK. Intracranial vascular stenosis and occlusion: evaluation with three-dimensional time-of-flight MR angiography. Radiology 1992;185:667–673 - PubMed
-
- Korogi Y, Takahashi M, Mabuchi N, et al. Intracranial vascular stenosis and occlusion: diagnostic accuracy of three-dimensional, Fourier transform, time-of-flight MR angiography. Radiology 1994;193:187–193 - PubMed
-
- Dagirmanjian A, Ross JS, Obuchowski N, et al. High resolution, magnetization transfer saturation, variable flip angle, time-of-flight MRA in the detection of intracranial vascular stenoses. J Comput Assist Tomogr 1995;19:700–706 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical