

Analysis of the cerebral cortex in holoprosencephaly with attention to the sylvian fissures
- PMID: 11827887
- PMCID: PMC7975520
Analysis of the cerebral cortex in holoprosencephaly with attention to the sylvian fissures
Abstract
Background and purpose: Analysis of specific features in the brain of patients with holoprosencephaly (HPE) may clarify normal and abnormal brain development and help predict outcomes for specific children. We assessed sulcal and gyral patterns of cerebral cortex in patients with HPE and developed a method of grading brain development.
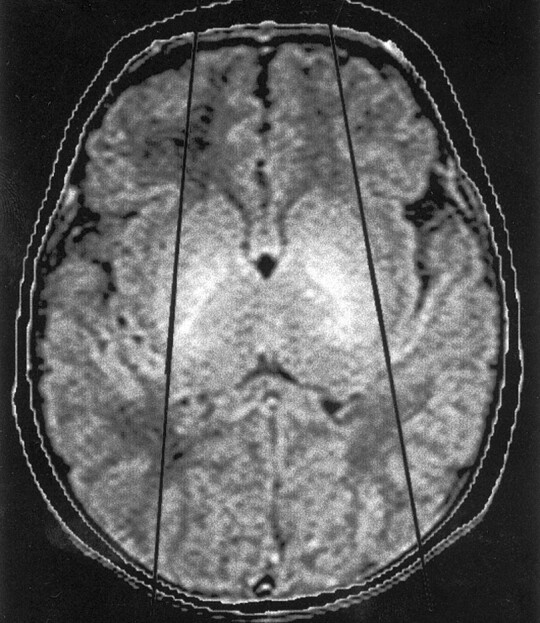
Methods: Neuroimaging studies (75 MR imaging, 21 CT) of 96 patients with HPE were retrospectively reviewed, with specific attention paid to the cerebral cortex. Thickness of cortex, width of gyri, and depth of sulci were assessed subjectively and by measurement. The angle between lines drawn tangential to the sylvian fissures ("sylvian angle") was measured in each patient with HPE and in 20 control patients.
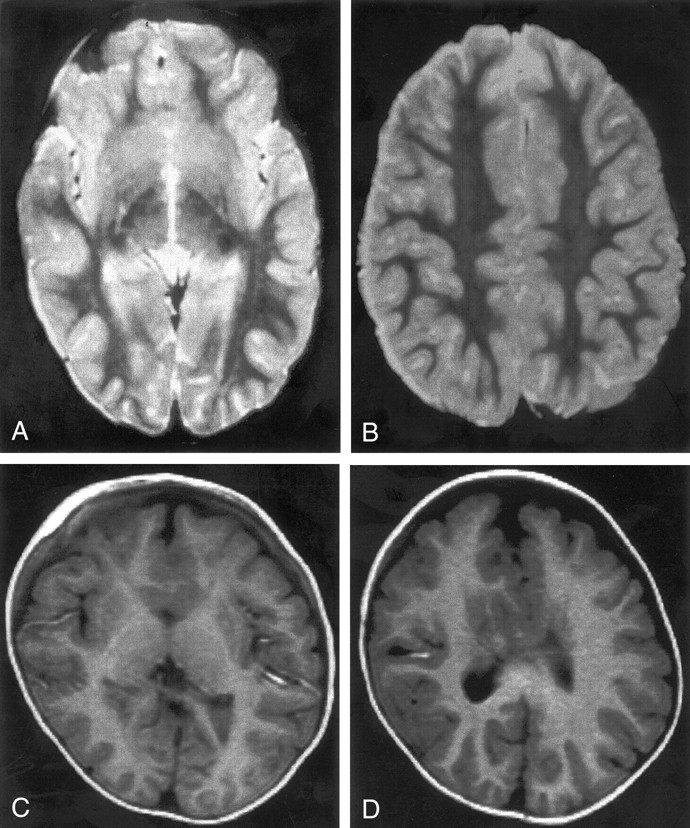
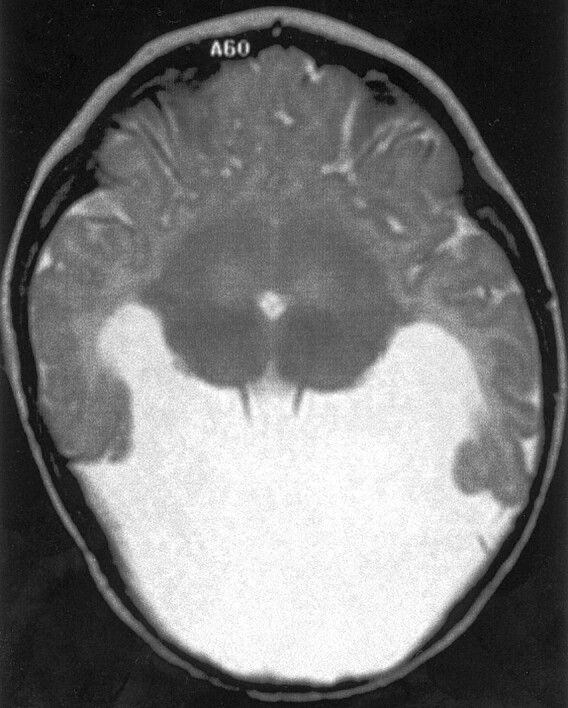
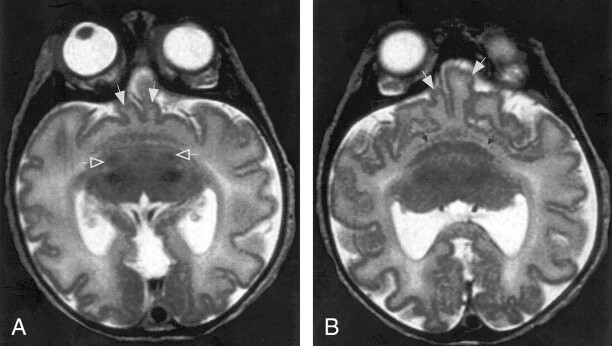
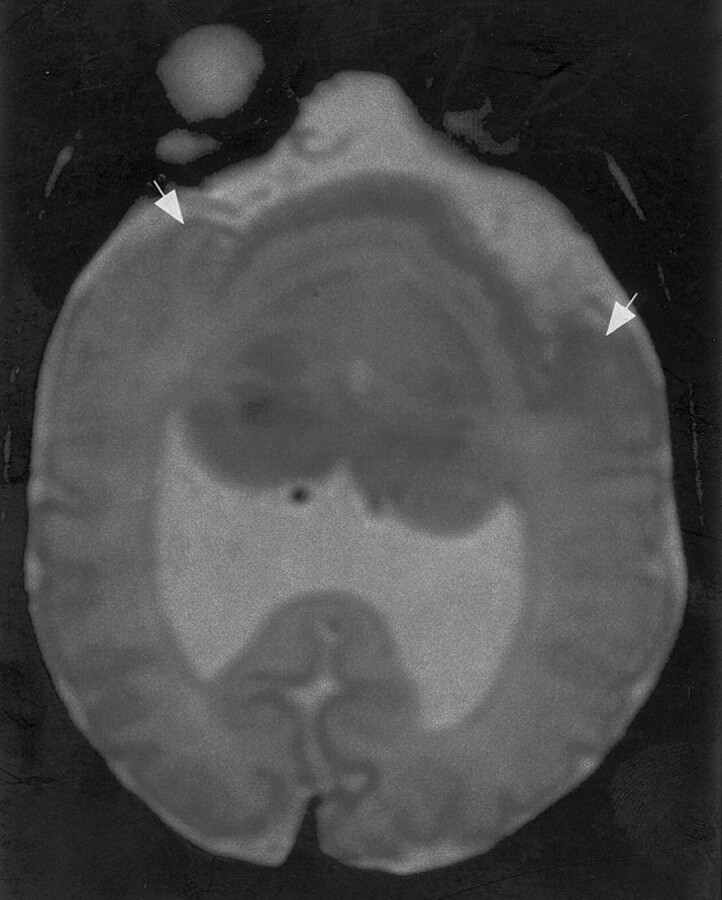
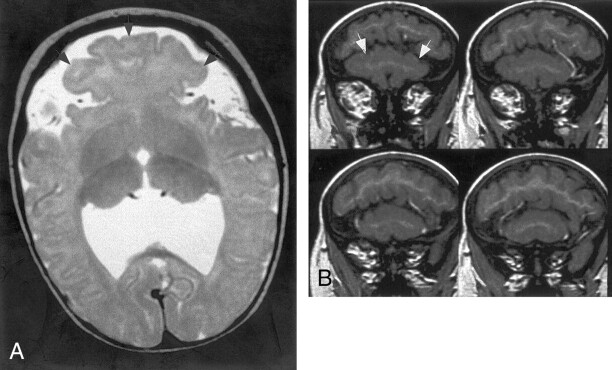
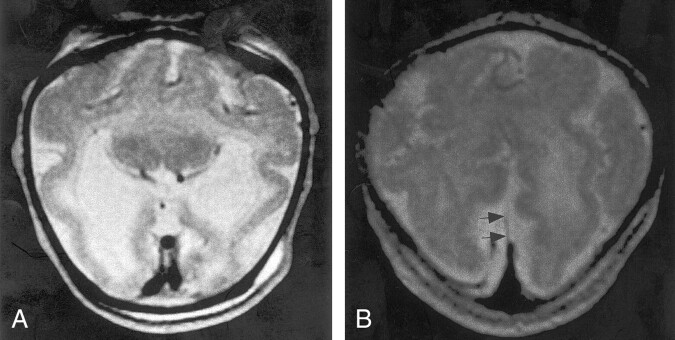
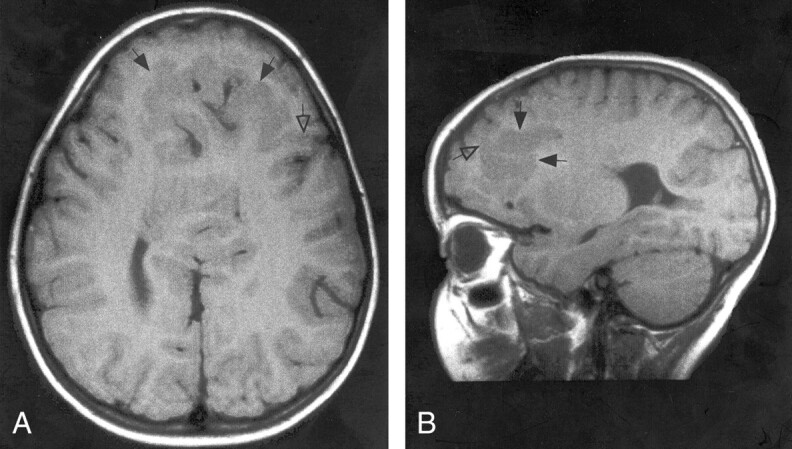
Results: Thickness of cortex was normal in all 96 patients. Gyral shape and width and sulcal depth were normal in 80 patients. Twelve patients, all with very severe HPE and microcephaly, had reduced sulcal depth, diffusely in eight and limited to the anteromedial cortex in four with lobar HPE. Four patients had subcortical heterotopia, located anterior to the interhemispheric fissure, associated with shallow sulci in the overlying cortex. Sylvian fissures were displaced further anteriorly and medially as HPE became more severe, until, in the most severe cases, no sylvian fissures could be identified. Sylvian angle measurements corresponded closely with severity of HPE, being largest in the most severe and smallest in the least severe cases. All patients with HPE had sylvian angles significantly larger than the mean of 15 degrees measured in the control patients.
Conclusion: The only true malformations of cortical development were subcortical heterotopia. However, diffuse and focal abnormal sulci were observed. We propose our sylvian angle measurement of extent of frontal lobe development as an objective means of quantifying the severity of HPE.
Figures

References
-
- DeMyer W. Holoprosencephaly (cyclopia-arhinencephaly). In: Myrianthopoulos N, ed. Malformations. New York: Elsevier;1987. :225–244
-
- DeMyer W, Zeman W. Alobar holoprosencephaly (arhinencephaly) with median cleft lip and palate: clinical, nosologic, and electroencephalographic considerations. Confin Neurol 1963;23:1–36 - PubMed
-
- DeMyer W, Zeman W, Palmer CG. The face predicts the brain: diagnostic significance of median facial anomalies for holoprosencephaly (arhinencephaly). Pediatrics 1964;34:256–263 - PubMed
-
- Probst FP. The Prosencephalies: Morphology, Neuroradiological Appearances and Differential Diagnosis. Berlin: Springer-Verlag; 1979:46
-
- Golden JA. Towards a greater understanding of the pathogenesis of holoprosencephaly. Brain Dev 1999;21:513–521 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical