

Effects of reduced mucus oxygen concentration in airway Pseudomonas infections of cystic fibrosis patients
- PMID: 11827991
- PMCID: PMC150856
- DOI: 10.1172/JCI13870
Effects of reduced mucus oxygen concentration in airway Pseudomonas infections of cystic fibrosis patients
Abstract
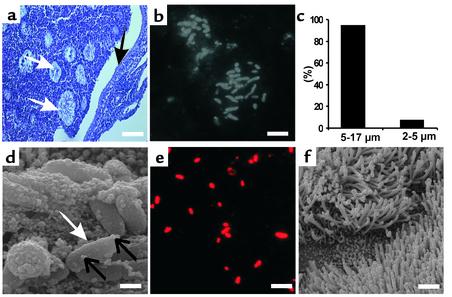
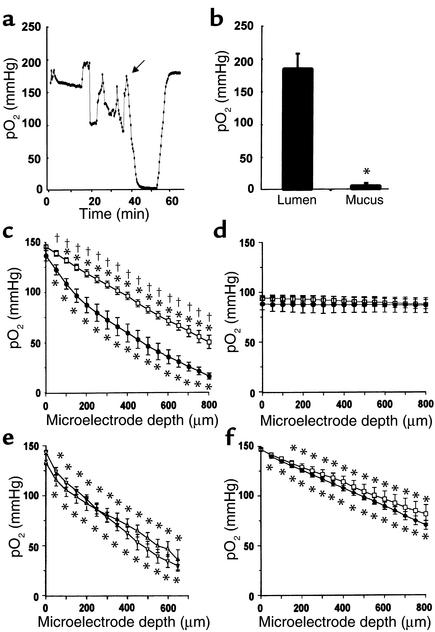
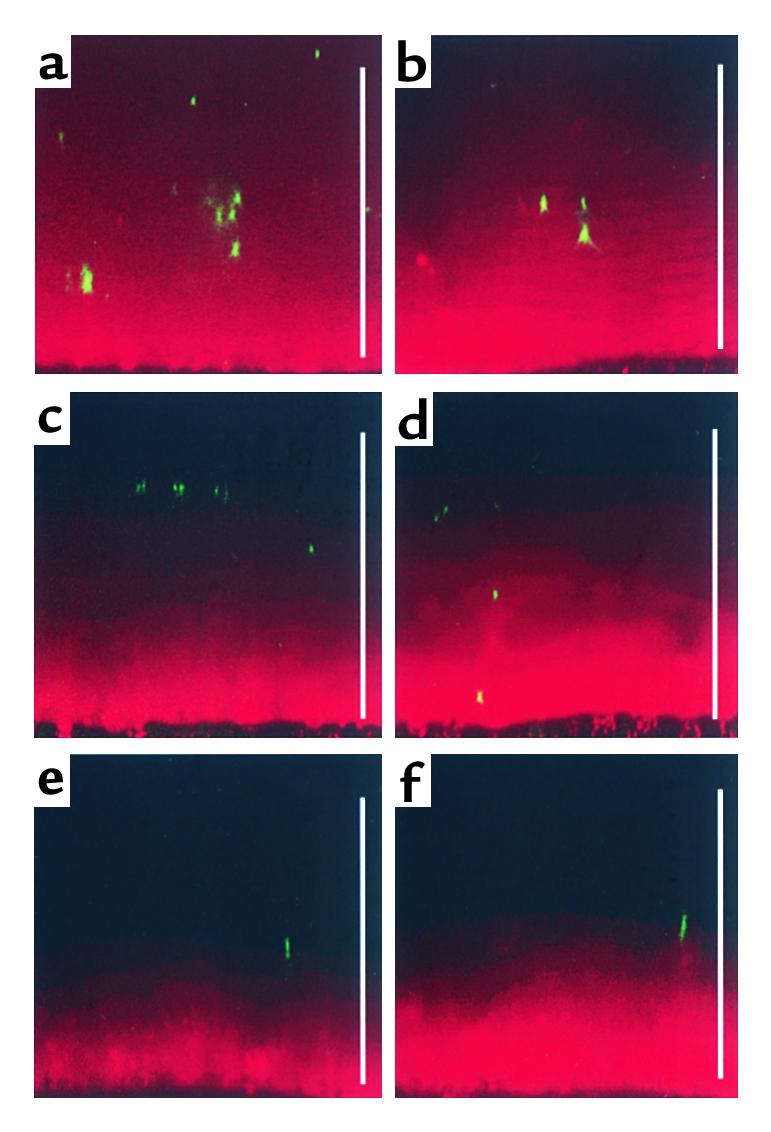
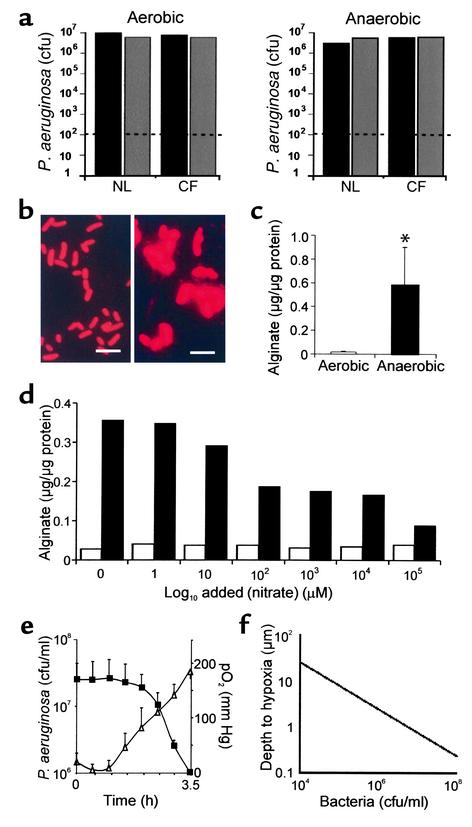
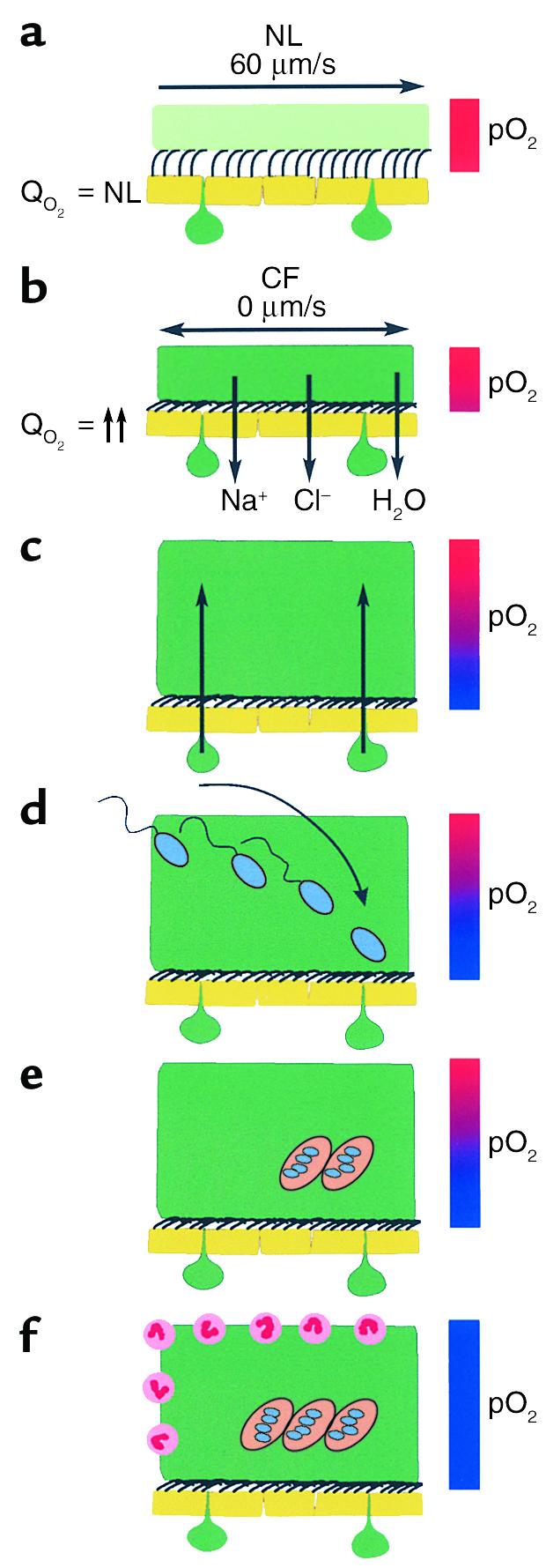
Current theories of CF pathogenesis predict different predisposing "local environmental" conditions and sites of bacterial infection within CF airways. Here we show that, in CF patients with established lung disease, Pseudomonas aeruginosa was located within hypoxic mucopurulent masses in airway lumens. In vitro studies revealed that CF-specific increases in epithelial O(2) consumption, linked to increased airway surface liquid (ASL) volume absorption and mucus stasis, generated steep hypoxic gradients within thickened mucus on CF epithelial surfaces prior to infection. Motile P. aeruginosa deposited on CF airway surfaces penetrated into hypoxic mucus zones and responded to this environment with increased alginate production. With P. aeruginosa growth in oxygen restricted environments, local hypoxia was exacerbated and frank anaerobiosis, as detected in vivo, resulted. These studies indicate that novel therapies for CF include removal of hypoxic mucus plaques and antibiotics effective against P. aeruginosa adapted to anaerobic environments.
Figures
References
-
- Davis PB, Drumm M, Konstan MW. Cystic fibrosis. Am J Respir Crit Care Med. 1996;154:1229–1256. - PubMed
-
- Meyer KC, Zimmerman J. Neutrophil mediators, Pseudomonas, and pulmonary dysfunction in cystic fibrosis. J Lab Clin Med. 1993;121:654–661. - PubMed
-
- Doering, G., Knight, R., and Bellon, G. 2000. Immunology of cystic fibrosis. In Cystic fibrosis. M.E. Hodson and D.M. Geddes, editors. Arnold Publishers. London, United Kingdom. 109–140.
-
- de Bentzmann S, Plotkowski C, Puchelle E. Receptors in the Pseudomonas aeruginosaadherence to injured and repairing airway epithelium. Am J Respir Crit Care Med. 1996;154:S155–S162. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
