

Epidemiological differences between adenocarcinoma of the oesophagus and adenocarcinoma of the gastric cardia in the USA
- PMID: 11839716
- PMCID: PMC1773122
- DOI: 10.1136/gut.50.3.368
Epidemiological differences between adenocarcinoma of the oesophagus and adenocarcinoma of the gastric cardia in the USA
Abstract
Background and aims: It has been suggested that gastric cardia adenocarcinoma (GCA) is a distinct entity from oesophageal adenocarcinoma (OA). We examined several epidemiological features of GCA and OA in the USA to elucidate differences/similarities between these malignancies.
Methods: Using the database of Surveillance, Epidemiology, and End Results (SEER) program, we examined incidence rates for temporal changes, and ethnic and age distributions, and performed birth cohort analyses for cases with morphologically and histologically confirmed OA or GCA.
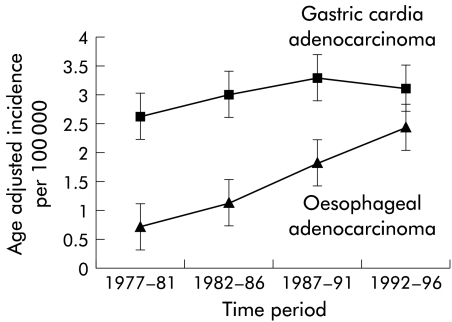
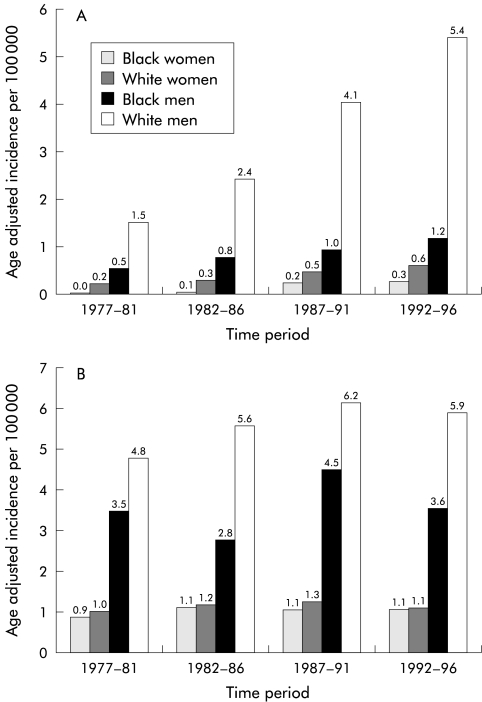
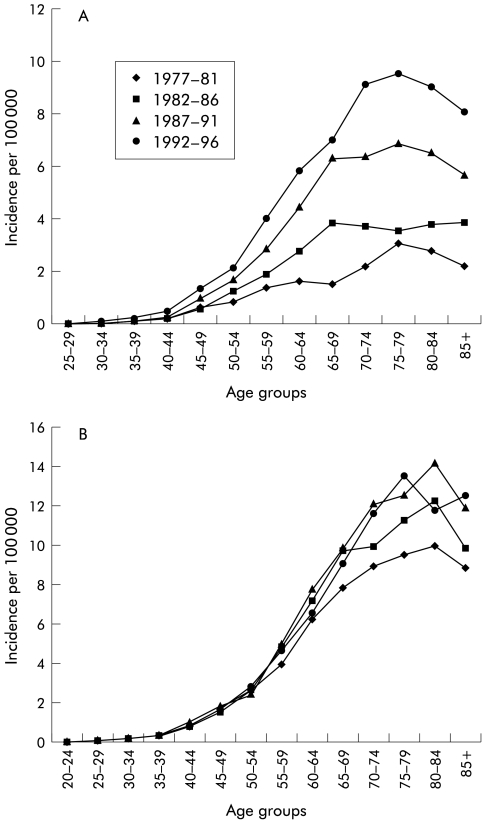
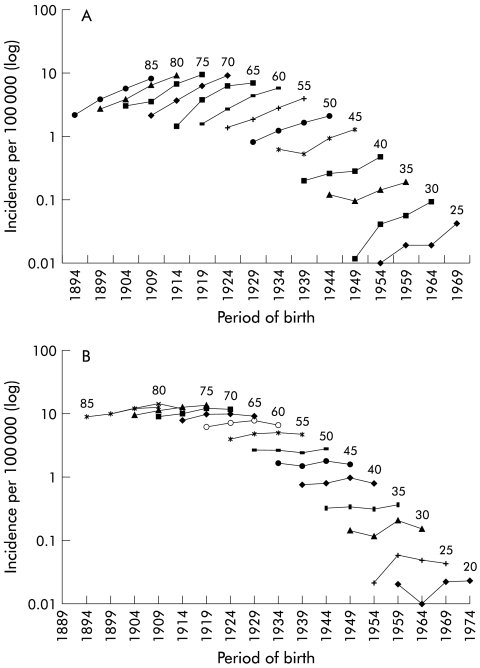
Results: The age adjusted incidence rates of OA rose progressively, reaching 1.8 per 100 000 (95% confidence interval 1.7-1.9) during 1987-1991 and 2.5 per 100 000 (2.3-2.6) during 1992-1996. In 1992-1996, Whites were affected five times more than Blacks, and men eight times more than women. A significant increase in incidence occurred among younger persons aged 45-65 years. Irrespective of age, OA was characterised by higher incidence rates among more recent birth cohorts: a 40% increase in incidence for each five year increase in the date of birth--a "birth cohort effect". On the other hand, the incidence rates of GCA reached their highest level of 3.3 per 100 000 (3.2-3.4) in 1987-1991 and subsequently declined during 1992-1996 to 3.1 per 100 000 (3.0-3.3). Whites were affected twice more than blacks and men five times more than women. Most patients with GCA were older than 60 years with no increase among younger persons and no birth cohort effect (p=0.99).
Conclusion: Several significant epidemiological differences exist between OA and GCA. These differences suggest that these two malignancies are separate entities with different risk factors.
Figures
References
-
- Blot WJ, Devesa SS, Kneller RW, et al. Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA 1991;265:1287–9. - PubMed
-
- Devesa SS, Blot WJ, Fraumeni JF Jr. Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer 1998;83:2049–53. - PubMed
-
- Spechler SJ, Goyal RK. Barrett's esophagus. N Engl J Med 1986;315: 362–71. - PubMed
-
- Graham DY, Yamakoa Y. H. pylori and CagA: relationships with gastric cancer, duodenal ulcer, and reflux esophagitis and its complications. Helicobacter 1998;3:145–51. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical