

Perineural tumor spread along the auriculotemporal nerve
- PMID: 11847060
- PMCID: PMC7975246
Perineural tumor spread along the auriculotemporal nerve
Abstract
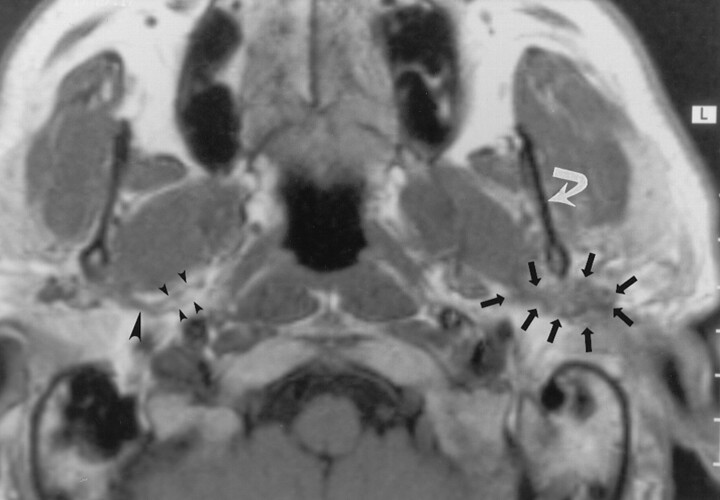
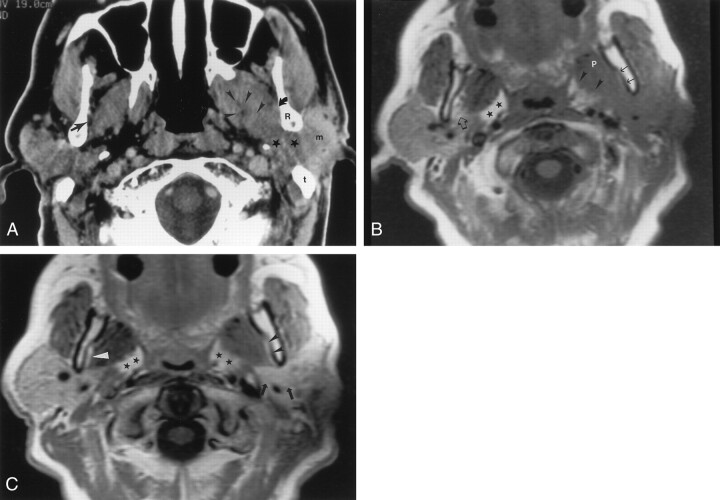
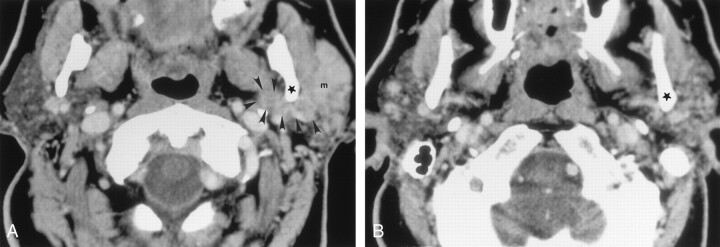
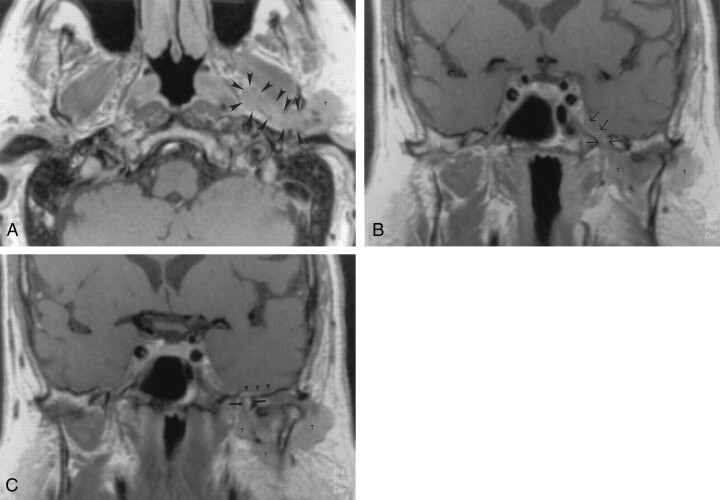
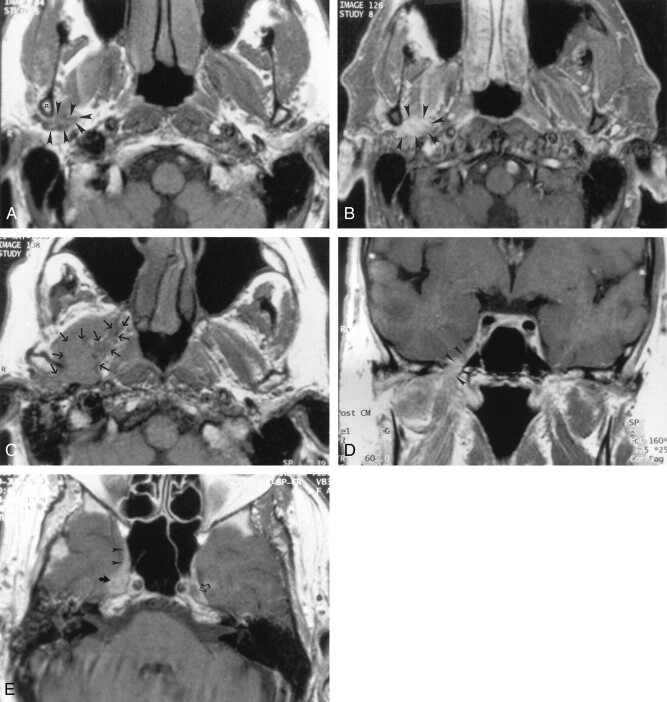
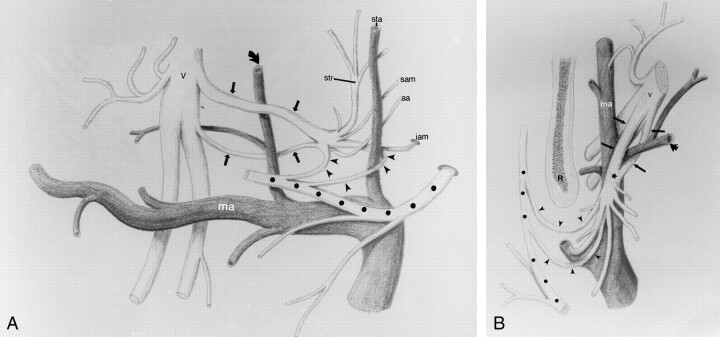
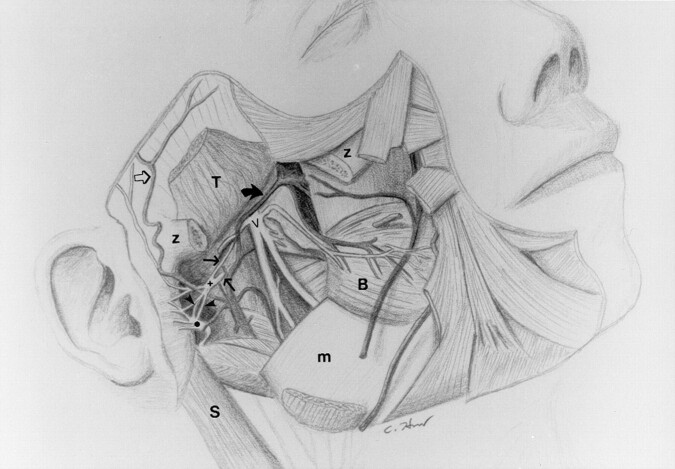
Background and purpose: Evaluation of images of perineural tumor spread in patients with head and neck malignancies is essential for planning treatment and determining the patient's prognosis. Although the communications between the facial and trigeminal nerves are not widely known, they may provide a route for tumor growth. The purpose of this study was to elucidate the course of the auriculotemporal nerve, as well as the clinical and imaging findings that suggest involvement of the communication between the facial nerve and the mandibular division (V(3)) of the trigeminal nerve.
Methods: Images in 15 patients with clinical or radiologic findings suggestive of perineural tumor spread along the auriculotemporal nerve were reviewed. Involvement of the main trunk of the facial nerve, auriculotemporal nerve, V(3), trigeminal cistern, and ganglion and adjacent anatomic structures were noted in each patient.
Results: The course of the auriculotemporal nerve was described in detail. More than 50% of patients with perineural tumor spread along the auriculotemporal nerve had clinical signs of auriculotemporal nerve dysfunction, including periauricular pain and temporomandibular joint (TMJ) dysfunction or tenderness. Images in 13 of 15 patients with such tumor spread demonstrated findings of tumor growth along V(3.).
Conclusion: Knowledge of the course of the auriculotemporal nerve is critical in evaluating images for findings of tumor spread along this nerve. Periauricular pain, TMJ dysfunction or tenderness, and imaging signs of V(3) involvement are important indicators of potential involvement of the auriculotemporal nerve.
Figures
References
-
- Williams LS, Mancuso AA, Mendehall WM. Perineural spread of cutaneous squamous and basal cell carcinoma: CT and MR detection and its impact on patient management and prognosis. Int J Radiation Oncol Biol Physics 2001;49:1061–1069 - PubMed
-
- Ginsberg LE. Imaging of perineural tumor spread in head and neck cancer. Semin Ultrasound CT MRI 1999;20:175–186 - PubMed
-
- Curtin HD, Wolfe P, Snyderman N. The facial nerve between the styloid foramen and the parotid: computed tomographic imaging. Radiology 1983;149:165–169 - PubMed
-
- Caldemeyer KS, Mathews VP, Righi PD, Smith RR. Imaging features and clinical significance of perineural spread or extension of head and neck tumors. Radiographics 1998;18:97–110 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical