

Virtual coronary angioscopy using multislice computed tomography
- PMID: 11847152
- PMCID: PMC1767040
- DOI: 10.1136/heart.87.3.205
Virtual coronary angioscopy using multislice computed tomography
Abstract
Background: With faster image acquisition times and thinner slice widths, multislice detector computed tomography (MSCT) allows visualisation of human coronary arteries with diagnostic image quality. In addition to conventional axial slices, virtual coronary angioscopies (VCA) can be reconstructed using MSCT datasets.
Objective: To evaluate the feasibility of reconstructing VCA and to determine the clinical value of this new application in detecting atherosclerotic coronary artery lesions.
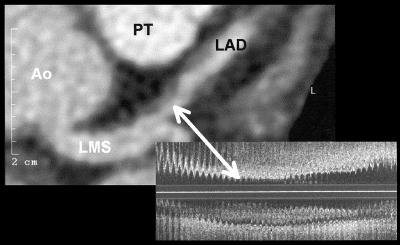
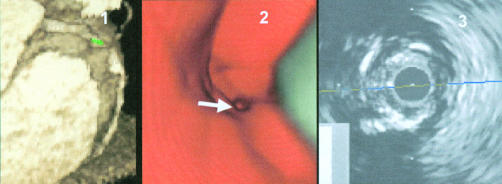
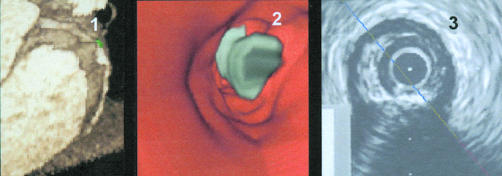
Methods: Datasets obtained by contrast enhanced non-invasive coronary angiography using MSCT (Somatom VZ) were analysed from 14 consecutive patients. VCA were simulated in 14 coronary arteries (left anterior descending, n = 7; right coronary, n = 7). Lesion detection was undertaken on conventional contrast enhanced axial slices, as well as by VCA. Intracoronary ultrasound (ICUS) was used as the gold standard for in vivo plaque detection.
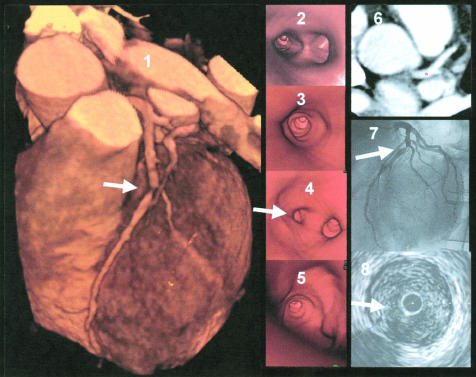
Results: 38 lesions were detected both on ICUS and on axial slices: 14 severe target lesions of > 75% area stenosis (11 calcified, three non-calcified), and 24 intermediate lesions of < or = 75% area stenosis (seven calcified, 17 non-calcified). Using VCA, all severe lesions (n = 14) and all calcified intermediate plaques (n = 7) could clearly be identified. However, non-calcified intermediate lesions (n = 17) could not be accurately distinguished from the vessel wall; they were recognised as vessel wall alterations without significant luminal narrowing.
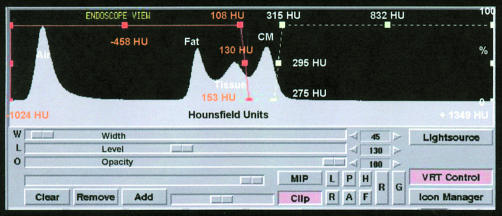
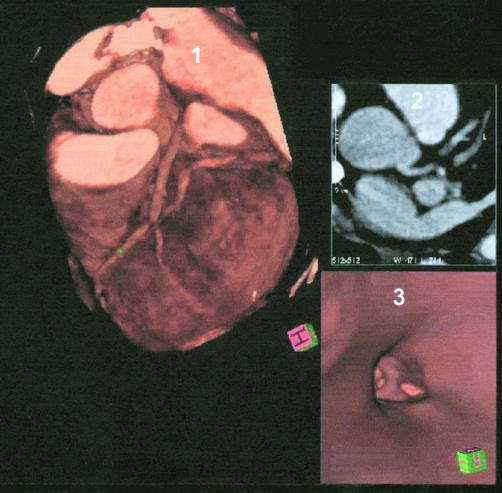
Conclusions: Current MSCT technology allows reconstruction of VCA with good image quality. Despite a more anatomical view of heart and coronary vessels on three dimensional reconstruction, conventional axial slices were found to be superior for detecting coronary lesions. Thus further technical innovations are required before VCA can become a useful technique in clinical cardiology.
Figures

Comment in
-
New coronary imaging techniques: what to expect?Heart. 2002 Mar;87(3):195-7. doi: 10.1136/heart.87.3.195. Heart. 2002. PMID: 11847148 Free PMC article. No abstract available.
References
-
- Ackerman JD. Medicine meets virtual reality 2000. MD Comput 2000;17:13–17. - PubMed
-
- Fletcher JG, Luboldt W. CT colonography and MR colonography: current status, research directions and comparison. Eur Radiol 2000;10:786–801. - PubMed
-
- Potchen EJ. Prospects for progress in diagnostic imaging. J Intern Med 2000;247:411–24. - PubMed
-
- Ott DJ. Virtual gastroscopy: a new look at the stomach. Am J Gastroenterol 2000;95:1084–5. - PubMed
-
- Chaoui AS, Blake MA, Barish MA, et al. Virtual colonoscopy and colorectal cancer screening. Abdom Imaging 2000;25:361–7. - PubMed