

Natural history of growth of secundum atrial septal defects and implications for transcatheter closure
- PMID: 11847166
- PMCID: PMC1767041
- DOI: 10.1136/heart.87.3.256
Natural history of growth of secundum atrial septal defects and implications for transcatheter closure
Abstract
Objective: To investigate the natural history of secundum atrial septal defects (ASDs) over several years using serial echocardiographic studies.
Methods: All patients with isolated secundum ASDs who had serial transthoracic echocardiograms at Texas Children's Hospital, Houston, Texas, from January 1991 to December 1998 were identified. Patients with fenestrated or multiple ASDs, other congenital heart defects, or less than a six month interval between echocardiograms were excluded. There were 104 patients eligible for inclusion in the study. Studies were reviewed by two echocardiographers (blinded) and the maximal diameter was recorded. Defects were defined as small (> 3 mm to < 6 mm), moderate (> or = 6 mm to < 12 mm), or large (> or = 12 mm). ASDs that grew > or = 20 mm were defined as having outgrown transcatheter closure with the device available to the authors' institution.
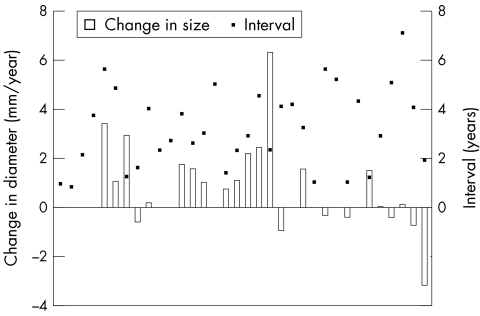
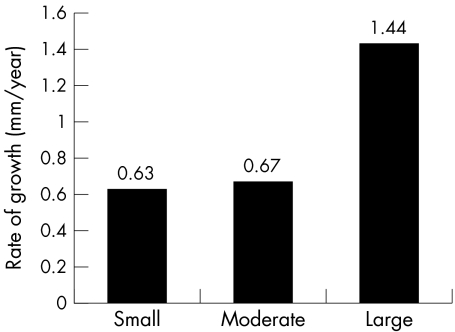
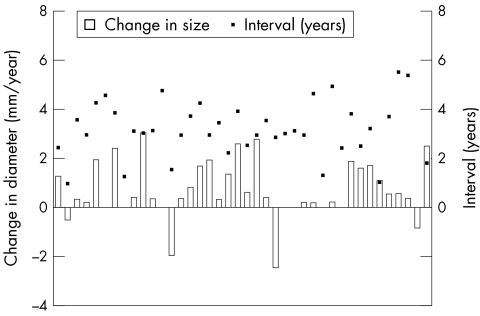
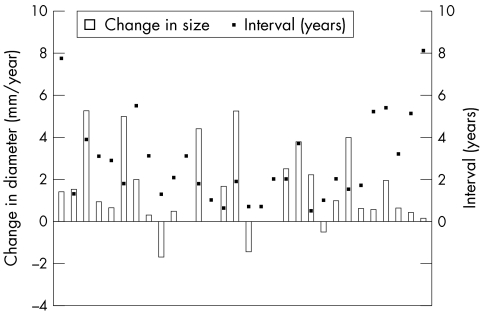
Results: ASD diameter increased in 68 of 104 patients (65%), including 31 patients (30%) with a > 50% increase in diameter. Spontaneous closure occurred in four patients (4%). Thirteen defects (12%) increased to > or = 20 mm. One fifth of the patients studied had an insufficient atrial rim by transthoracic echocardiogram to hold an atrial septal occluder. The only factor associated with significant growth of ASDs was initial size of the defect. ASD growth was independent both of age at diagnosis and when indexed to body surface area.
Conclusions: Two thirds of secundum ASDs may enlarge with time and there is the potential for secundum ASDs to outgrow transcatheter closure with specific devices. Further development in devices and general availability of devices capable of closing larger ASDs should circumvent this problem.
Figures
References
-
- Radzik D, Davignon A, von Doesburg N, et al. Predictive factors for spontaneous closure of atrial septal defects diagnosed in the first 3 months of life. J Am Coll Cardiol 1993;22:851–3. - PubMed
-
- Helgason H, Jonsdottir G. Spontaneous closure of atrial septal defects. Pediatr Cardiol 1999;20:195–9. - PubMed
-
- Brassard M, Fouron JC, van Doesburg NH, et al. Outcome of children with atrial septal defect considered too small for surgical closure. Am J Cardiol 1999;83:1552–5. - PubMed
-
- Hartmann AF, Elliott LP. Spontaneous physiologic closure of an atrial septal defect after infancy. Am J Cardiol 1967;19:290–2. - PubMed
-
- Fukasawa M, Fukushige J, Ueda K. Atrial septal defect in neonates with reference to spontaneous closure. Am Heart J 1988;116:123–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources