

Review
doi: 10.1136/heart.87.3.299.
Which patient should be referred to an electrophysiologist: supraventricular tachycardia
Affiliations
- PMID: 11847181
- PMCID: PMC1767049
- DOI: 10.1136/heart.87.3.299
Item in Clipboard
Review
Which patient should be referred to an electrophysiologist: supraventricular tachycardia
Heart.
2002 Mar.
No abstract available
Figures
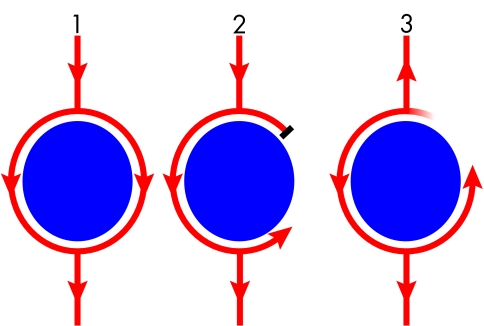
Diagrammatic representation of the mechanisms of re-entry. (1) A wavefront (arrows), initiated in a normal fashion in the sinus node, passes around an obstacle (disc) to electrical activation in a uniform fashion. This obstacle may be formed by an anatomical feature (fixed conduction block) like the tricuspid annulus, or by a physiological abnormality (functional conduction block) like an area of ischaemic myocardium, which may or may not result in block depending on a variety of conditions like vagal tone or coupling interval. (2) A premature impulse results in block of conduction on one side of the obstacle while conduction continues on the other. This is functional block because it is the result of a short electrical coupling interval which means that the myocardium in this region has not recovered its excitability in time to conduct the premature beat. (3) This wavefront takes sufficient time to circulate around the obstacle that repolarisation occurs and the area previously resulting in block recovers its excitability, so that this wavefront continually encounters excitable tissue and perpetuates as a re-entry circuit.
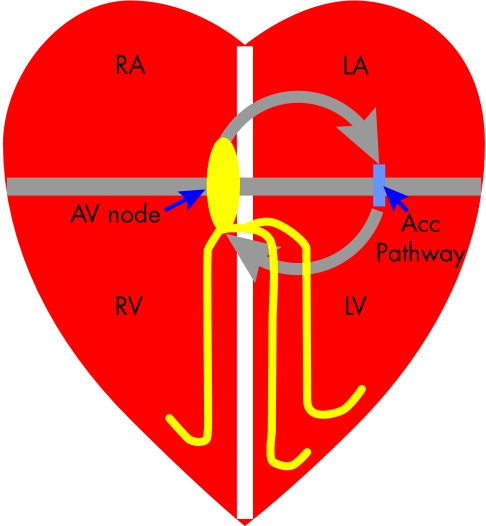
Mechanism of atrioventricular re-entry tachycardias (AVRT). The right and left atria (RA/LA) and ventricles (RV/LV) are normally electrically isolated by the fibrous rings that form the mitral and tricuspid annulus (grey line), with the only connection being the atrioventricular (AV) node. If a patient has an accessory connection (acc pathway) then the requirements for a re-entry circuit (grey arrows) are fulfilled; where the mitral/tricuspid annuli form fixed conduction block and the AV node, accessory pathway and tissue of the atria and ventricles form the re-entry circuit.
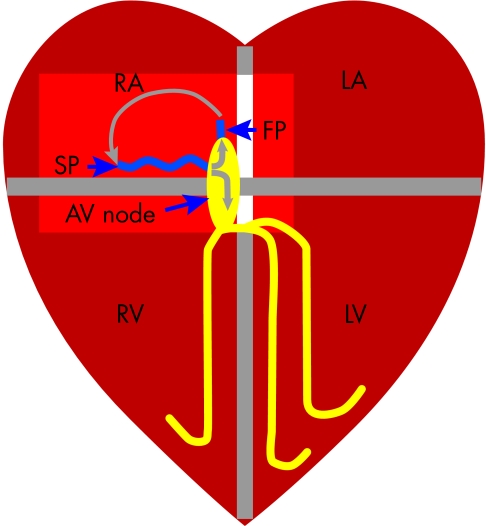
Mechanism of atrioventricular nodal re-entry tachycardia (AVNRT). Patients with AVNRT have two inputs to the AV node—a slow (SP) and fast (FP) pathway. The re-entry circuit is formed by the SP, AV node, FP and the atrial tissue intervening between the FP and SP, and most commonly activates in the direction shown by the grey arrows. Note that the ventricle activates via the AV node but is not part of the re-entry circuit (unlike in AVRT). Adenosine will block conduction through the AV node, which is part of the re-entry circuit in both AVNRT and AVRT and therefore terminates the tachycardia.
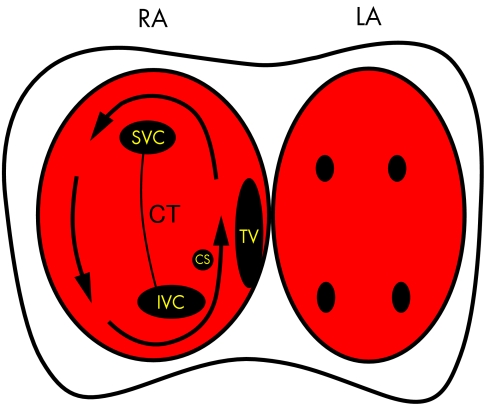
Diagram showing the pathway taken by the re-entry wavefront causing atrial flutter (arrow). The right (RA) and left atria (LA) are depicted with the anatomical landmarks in the right atria marked as follows: SVC, superior vena cava; IVC, inferior vena cava; CS, coronary sinus os; TV, tricuspid valve; CT, crista terminalis. The TV and CT form lines of conduction block which “electrically” divide the atria into two halves. The only electrical connections between these two halves are the roof and appendage of the right atrium and the isthmus between the TV and IVC. Note that the narrowest part of the re-entry circuit is this isthmus which is why this is the target for ablation of atrial flutter. The left atrium activates via conduction through the septum but is not part of the re-entry circuit.
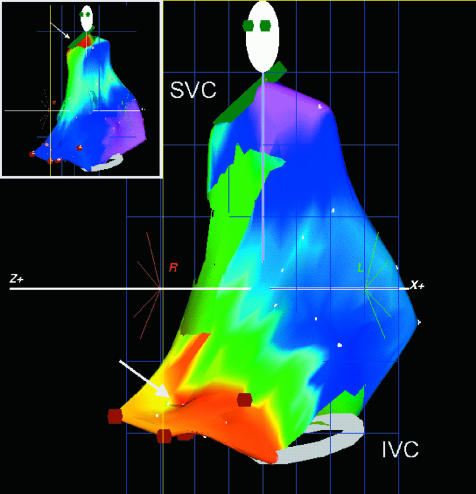
An electroanatomical map of the right atrium in a patient with focal atrial tachycardia (AT). The atrium is shown in the left anterior oblique (LAO) view with the superior (SVC) and inferior vena cava (IVC) shown as rings on the map. An isochronal map has been superimposed onto the computer generated model of the right atrium. This shows early activation in red and latest activation in purple. The earliest activation can be seen at the low lateral right atrium which is in contrast to activation during sinus rhythm (inset) which is earliest at the superior lateral right atrium, the location of the sinus node.
References
-
- Jackman WM, Beckman KJ, McClelland JH, et al. Treatment of supraventricular tachycardia due to atrioventricular nodal reentry, by radiofrequency catheter ablation of slow-pathway conduction. N Engl J Med 1992;327:313–8. ▸ This is the first description of the technique of slow pathway ablation for treating AVNRT, one of the more common regular SVTs. It proved to be easier to perform and have fewer complications than the previous approach of fast pathway ablation, and as such revolutionised the treatment of patients with AVNRT. - PubMed
-
- Tai CT, Chen SA, Chiang CE, et al. Characterization of low right atrial isthmus as the slow conduction zone and pharmacological target in typical atrial flutter. Circulation 1997;96:2601–11. - PubMed
-
- Shah DC, Jaïs P, Haïssaguerre M, et al. Three-dimensional mapping of the common atrial flutter circuit in the right atrium. Circulation 1997;96:3904–12. - PubMed
-
- Kinder C, Kall J, Kopp D, et al. Conduction properties of the inferior vena cava-tricuspid annular isthmus in patients with typical atrial flutter. J Cardiovasc Electrophysiol 1997;8:727–37. - PubMed
-
- Saoudi N, Cosio F, Waldo A, et al. Classification of atrial flutter and regular atrial tachycardia according to electrophysiologic mechanism and anatomic bases: a statement from a joint expert group from the working group of arrhythmias of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. J Cardiovasc Electrophysiol 2001;2:852–66 . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources