

Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study
- PMID: 11850367
- PMCID: PMC65530
- DOI: 10.1136/bmj.324.7334.387
Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study
Abstract
Objectives: To determine whether earlier clinical intervention by a medical emergency team prompted by clinical instability in a patient could reduce the incidence of and mortality from unexpected cardiac arrest in hospital.
Design: A non-randomised, population based study before (1996) and after (1999) introduction of the medical emergency team.
Setting: 300 bed tertiary referral teaching hospital.
Participants: All patients admitted to the hospital in 1996 (n=19 317) and 1999 (n=22 847).
Interventions: Medical emergency team (two doctors and one senior intensive care nurse) attended clinically unstable patients immediately with resuscitation drugs, fluid, and equipment. Response activated by the bedside nurse or doctor according to predefined criteria.
Main outcome measures: Incidence and outcome of unexpected cardiac arrest.
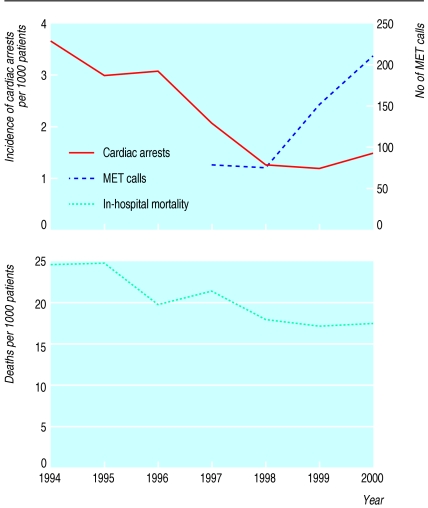
Results: The incidence of unexpected cardiac arrest was 3.77 per 1000 hospital admissions (73 cases) in 1996 (before intervention) and 2.05 per 1000 admissions (47 cases) in 1999 (after intervention), with mortality being 77% (56 patients) and 55% (26 patients), respectively. After adjustment for case mix the intervention was associated with a 50% reduction in the incidence of unexpected cardiac arrest (odds ratio 0.50, 95% confidence interval 0.35 to 0.73).
Conclusions: In clinically unstable inpatients early intervention by a medical emergency team significantly reduces the incidence of and mortality from unexpected cardiac arrest in hospital.
Figures
Comment in
-
Medical emergency teams and cardiac arrests in hospital. Results may have been due to education of ward staff.BMJ. 2002 May 18;324(7347):1215; author reply 1215. doi: 10.1136/bmj.324.7347.1215/a. BMJ. 2002. PMID: 12016195 Free PMC article. No abstract available.
-
Medical emergency teams and cardiac arrests in hospital. Bottom up approach works too.BMJ. 2002 May 18;324(7347):1215; author reply 1215. BMJ. 2002. PMID: 12018220 No abstract available.
References
-
- Brennan TA, Leape LL, Laird NM, Hebert L, Localio AR, Lawthers AG. Incidence of adverse events and negligence in hospitalized patients: results of the Harvard medical practice study I. N Engl J Med. 1991;324:370–376. - PubMed
-
- Wilson RM, Runciman WB, Gibberd RW, Harrrison BT, Newby L, Hamilton JD. The quality in Australian health care study. Med J Aust. 1995;163:458–471. - PubMed
-
- Leape LL, Brennan TA, Laird N, Lawthers Ag, Localio AR, Barnes BA. The nature of adverse events in hospitalized patients: results of the Harvard medical practice study II. N Engl J Med. 1991;324:377–384. - PubMed
-
- Wilson RM, Harrison BT, Gibberd RW, Hamilton JD. An analysis of the causes of adverse events from the quality in Australian health care study. Med J Aust. 1999;170:411–415. - PubMed
-
- Peatfield RC, Sillett RW, Taylor D, McNicol MW. Survival after cardiac arrest in hospital. Lancet. 1977;i:1223–1225. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical