

Heterogeneous proliferative potential of occult metastatic cells in bone marrow of patients with solid epithelial tumors
- PMID: 11854519
- PMCID: PMC122350
- DOI: 10.1073/pnas.042372199
Heterogeneous proliferative potential of occult metastatic cells in bone marrow of patients with solid epithelial tumors
Abstract
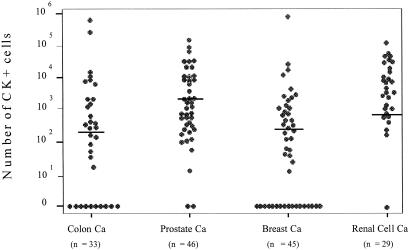
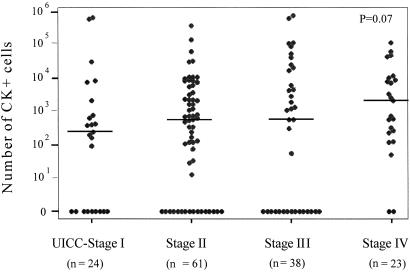
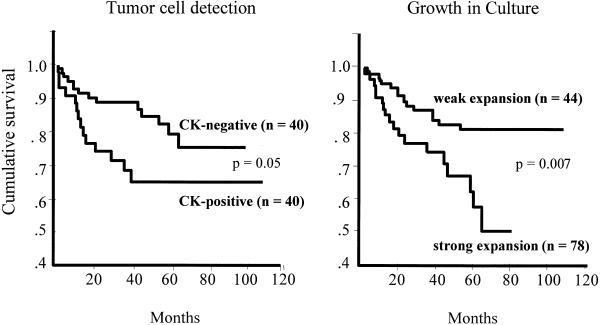
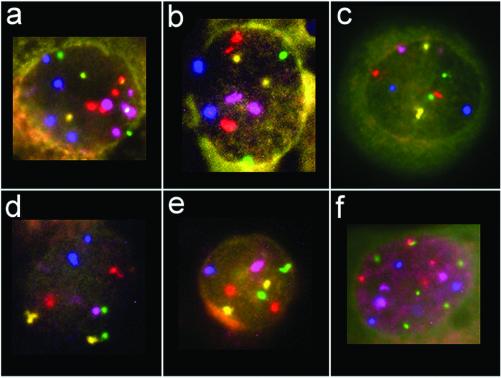
Bone marrow is a major homing site for circulating epithelial tumor cells. The present study was aimed to assess the proliferative capacity of occult metastatic cells in bone marrow of patients with operable solid tumors especially with regard to their clinical outcome. We obtained bone marrow aspirates from 153 patients with carcinomas of the prostate (n = 46), breast (n = 45), colon (n = 33), and kidney (n = 29). Most of the patients (87%) had primary disease with no clinical signs of overt metastases [tumor-node-metastasis (TNM)-stage UICC (Union Internationale Contre le Cancer) I-III]. After bone marrow was cultured for 21-102 days under special cell culture conditions, viable epithelial cells were detected by cytokeratin staining in 124 patients (81%). The cultured epithelial cells harbored Ki-ras2 mutations and numerical chromosomal aberrations. The highest median number of expanded tumor cells was observed in prostate cancer (2,619 per flask). There was a significant positive correlation between the number of expanded tumor cells and the UICC-stage of the patients (P = 0.03) or the presence of overt metastases (P = 0.04). Moreover, a strong expansion of tumor cells was correlated to an increased rate of cancer-related deaths (P = 0.007) and a reduced survival of the patients (P = 0.006). In conclusion, the majority of cancer patients have viable tumor cells in their bone marrow at primary tumor diagnosis, and the proliferative potential of these cells determines the clinical outcome.
Figures
References
-
- Pantel K, Cote R J, Fodstad Ø. J Natl Cancer Inst. 1999;91:1113–1124. - PubMed
-
- Lindemann F, Schlimok G, Dirschedl P, Witte J, Riethmüller G. Lancet. 1992;340:685–689. - PubMed
-
- Soeth E, Vogel I, Röder C, Juhl H, Marxsen J, Krüger U, Henne-Bruns D, Kremer B, Kalthoff H. Cancer Res. 1997;57:3106–3110. - PubMed
-
- Leinung S, Würl P, Schönfelder A, Weiss C-L, Röder I, Schönfelder M. J Hematother. 2000;9:905–911. - PubMed
-
- Pantel K, Schlimok G, Angstwurm M, Weckermann C, Schmaus W, Gath H, Passlick B, Izbicki J, Riethmüller G. J Hematother. 1994;3:165–173. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
