

Ethnic differences in invasive management of coronary disease: prospective cohort study of patients undergoing angiography
- PMID: 11872548
- PMCID: PMC67765
- DOI: 10.1136/bmj.324.7336.511
Ethnic differences in invasive management of coronary disease: prospective cohort study of patients undergoing angiography
Abstract
Objectives: To compare rates of revascularisation in south Asian and white patients undergoing coronary angiography in relation to the appropriateness of revascularisation and clinical outcome.
Design: Prospective cohort study of patients with two and a half years' follow up; appropriateness of revascularisation rated by nine experts with no knowledge of ethnicity of patient.
Setting: Tertiary cardiac centre in London with referral from five contiguous health authorities.
Participants: Consecutive patients (502 south Asian, 2974 white) undergoing coronary angiography in the appropriateness of coronary revascularisation study (ACRE).
Main outcome measures: Coronary revascularisation, non-fatal myocardial infarction, mortality.
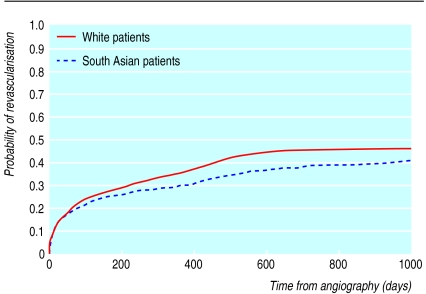
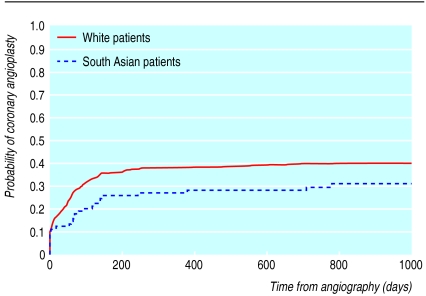
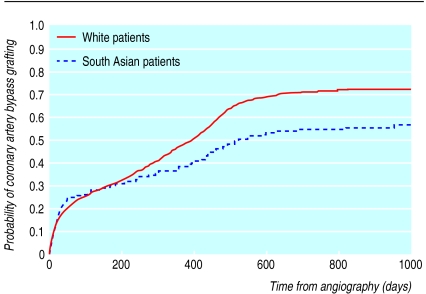
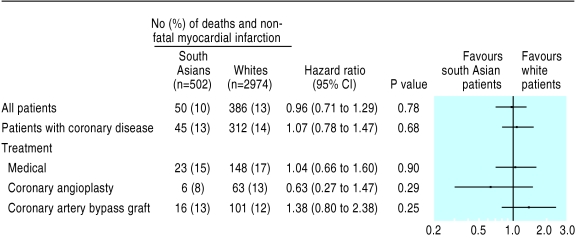
Results: There was no difference between south Asian and white patients in the proportions deemed appropriate for revascularisation (72% (361) v 68% (2022)) or in the proportions for whom the physician's intended management was revascularisation (39% (196) v 41% (1218)). Among patients appropriate for revascularisation, age adjusted rates of coronary angioplasty (hazard ratio 0.69, 95% confidence interval 0.47 to 1.00, P=0.058) and coronary artery bypass grafting (0.74, 0.58 to 0.91, P=0.007) were lower in south Asian than in white patients. These differences were smaller but still present after adjustment for socioeconomic status and after restriction of analysis to those patients for whom the intended management was revascularisation. There were no differences in mortality and non-fatal myocardial infarction between south Asian and white patients (1.07, 0.78 to 1.47).
Conclusion: Among patients deemed appropriate for coronary artery bypass grafting, south Asian patients are less likely than white patients to receive it. This difference is not explained by physician bias.
Figures
Comment in
-
Access to invasive procedures can be audited by ethnic group.BMJ. 2002 Jun 15;324(7351):1454. BMJ. 2002. PMID: 12065277 Free PMC article. No abstract available.
-
Heterogeneity among Indians, Pakistanis, and Bangladeshis is key to racial inequities.BMJ. 2002 Oct 19;325(7369):903. doi: 10.1136/bmj.325.7369.903/a. BMJ. 2002. PMID: 12386051 Free PMC article. No abstract available.
Similar articles
-
Hypothetical ratings of coronary angiography appropriateness: are they associated with actual angiographic findings, mortality, and revascularisation rate? The ACRE study.Heart. 2001 Jun;85(6):672-9. doi: 10.1136/heart.85.6.672. Heart. 2001. PMID: 11359750 Free PMC article.
-
Does access to cardiac investigation and treatment contribute to social and ethnic differences in coronary heart disease? Whitehall II prospective cohort study.BMJ. 2004 Aug 7;329(7461):318. doi: 10.1136/bmj.38156.690150.AE. Epub 2004 Jul 5. BMJ. 2004. PMID: 15237088 Free PMC article.
-
Coronary artery size and disease in UK South Asian and Caucasian men.Eur J Cardiothorac Surg. 2006 Apr;29(4):492-5. doi: 10.1016/j.ejcts.2006.01.008. Epub 2006 Feb 13. Eur J Cardiothorac Surg. 2006. PMID: 16473514
-
Invasive investigations and revascularisation.Br Med Bull. 2001;59:45-53. doi: 10.1093/bmb/59.1.45. Br Med Bull. 2001. PMID: 11756203 Review.
-
Evidence-based assessment of the benefit of revascularisation in coronary disease: beyond the randomised trials.Aust N Z J Med. 1996 Aug;26(4):490-4. doi: 10.1111/j.1445-5994.1996.tb00594.x. Aust N Z J Med. 1996. PMID: 8873931 Review. No abstract available.
Cited by
-
Likelihood of treatment in a coronary care unit for a first-time myocardial infarction in relation to sex, country of birth and socioeconomic position in Sweden.PLoS One. 2013 Apr 25;8(4):e62316. doi: 10.1371/journal.pone.0062316. Print 2013. PLoS One. 2013. PMID: 23638036 Free PMC article.
-
Ethnic differences in cardiovascular morbidity and mortality among patients with breast cancer in the Netherlands: a register-based cohort study.BMJ Open. 2018 Aug 17;8(8):e021509. doi: 10.1136/bmjopen-2018-021509. BMJ Open. 2018. PMID: 30121599 Free PMC article.
-
Ethnic disparities in coronary heart disease management and pay for performance in the UK.J Gen Intern Med. 2009 Jan;24(1):8-13. doi: 10.1007/s11606-008-0832-5. Epub 2008 Oct 25. J Gen Intern Med. 2009. PMID: 18953616 Free PMC article.
-
Ethnic differences between South Asians and White Caucasians in cardiovascular disease-related mortality in developed countries: a systematic literature review.Syst Rev. 2022 Sep 29;11(1):207. doi: 10.1186/s13643-022-02079-z. Syst Rev. 2022. PMID: 36176009 Free PMC article.
-
Short and long term mortality after coronary artery bypass grafting (CABG) is influenced by socioeconomic position but not by migration status in Sweden, 1995-2007.PLoS One. 2013 May 22;8(5):e63877. doi: 10.1371/journal.pone.0063877. Print 2013. PLoS One. 2013. PMID: 23717501 Free PMC article.
References
-
- Trevino FM. Quality of health care for ethnic/racial minority populations. Ethn Health. 1999;4:153–164. - PubMed
-
- Acheson D. Independent inquiry into inequalities in health report. London: Stationery Office; 1998.
-
- Fang J, Madhavan S, Alderman MH. The association between birthplace and mortality from cardiovascular causes among black and white residents of New York City. N Engl J Med. 1996;335:1545–1551. - PubMed
-
- Erens B, Primatesta P, Prior G. Health survey for England: the health of minority ethnic groups 1999. London: Stationery Office; 2001.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical