

Limitation of the in vitro whole blood assay for predicting the COX selectivity of NSAIDs in clinical use
- PMID: 11874389
- PMCID: PMC1874310
- DOI: 10.1046/j.0306-5251.2001.01533.x
Limitation of the in vitro whole blood assay for predicting the COX selectivity of NSAIDs in clinical use
Abstract
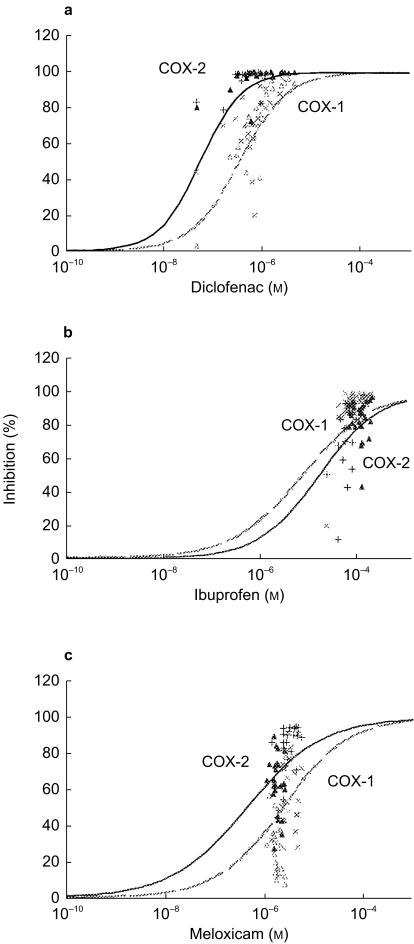
Aims: To assess if the inhibitory potency of nonsteroidal anti-inflammatory drugs (NSAIDs) on cyclooxygenase (COX) isoenzymes, when given therapeutically in humans, can be predicted from their in vitro concentration-response curves using the whole blood assay.
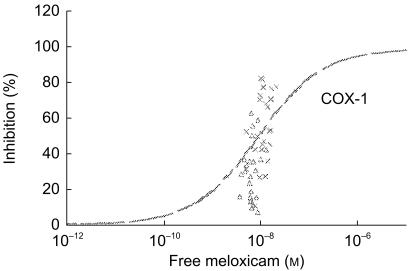
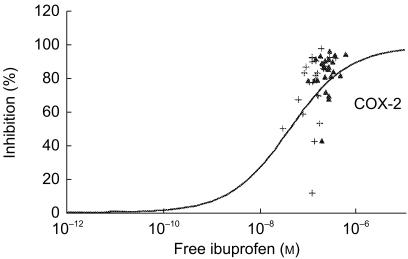
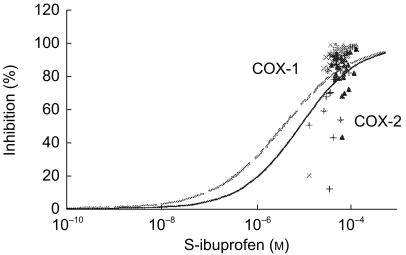
Methods: Twenty-four healthy male volunteers aged 20--27 years were recruited. Inhibition of blood COX isoenzymes was determined in vitro before any drug intake and ex vivo after single and repeated intake of either 7.5 mg meloxicam once, 400 mg ibuprofen three times daily or 75 mg diclofenac SR once, taken in a randomized cross-over design. Production of thromboxane B2 (TXB2) during clotting and of prostaglandin E2 (PGE2) during endotoxin exposure served as indicators of platelet COX-1 and monocyte COX-2 activity, respectively. Drugs were determined in plasma by h.p.l.c., with a chiral separation of ibuprofen and free fractions after equilibrium dialysis.
Results: Intra-subject variation for COX-1 and COX-2 at baseline was at 26 +/- 18% and 18 +/- 13% respectively, and intersubject variation at 39% and 36%, respectively. The ratios of IC50s and, at best, of IC80s revealed diclofenac and meloxicam as selective COX-2 inhibitors and ibuprofen as a preferential COX-1 inhibitor in vitro. However, after oral intake, ibuprofen inhibited ex vivo COX-2 by 80% whereas diclofenac inhibited COX-1 by 70%. Meloxicam inhibited COX-1 from 30 to 55% depending on the repetition of the dose and increase in plasma concentrations. Using in vitro dose--response curves, the in vivo inhibitory potency of diclofenac was estimated adequately from its circulating concentration ([-0.18, 0.21] for COX-1 and [-0.13, -0.03] for COX-2) but this was not the case for ibuprofen on COX-2 ([-0.14, 0.27]) and meloxicam on COX-1 ([0.31, 1.05]). The limited predictability of the system was not improved through considering the unbound fraction of the drugs or the variable chiral inversion of ibuprofen.
Conclusions: Assessment of COX-2 selectivity based on in vitro studies and pharmacological modelling has a limited clinical relevance. There is a need to investigate COX selectivity at therapeutic plasma concentrations of NSAIDs using the ex vivo whole blood assay.
Figures
Similar articles
-
Dose-dependent inhibition of platelet cyclooxygenase-1 and monocyte cyclooxygenase-2 by meloxicam in healthy subjects.J Pharmacol Exp Ther. 1999 Jul;290(1):276-80. J Pharmacol Exp Ther. 1999. PMID: 10381787 Clinical Trial.
-
Comparative inhibitory activity of rofecoxib, meloxicam, diclofenac, ibuprofen, and naproxen on COX-2 versus COX-1 in healthy volunteers.J Clin Pharmacol. 2000 Oct;40(10):1109-20. J Clin Pharmacol. 2000. PMID: 11028250 Clinical Trial.
-
A comparison of the effects of nabumetone vs meloxicam on serum thromboxane B2 and platelet function in healthy volunteers.Br J Clin Pharmacol. 2002 Jun;53(6):644-7. doi: 10.1046/j.1365-2125.2002.01605.x. Br J Clin Pharmacol. 2002. PMID: 12047490 Free PMC article. Clinical Trial.
-
Differentiating among nonsteroidal antiinflammatory drugs by pharmacokinetic and pharmacodynamic profiles.Semin Arthritis Rheum. 1997 Jun;26(6 Suppl 1):28-33. doi: 10.1016/s0049-0172(97)80050-9. Semin Arthritis Rheum. 1997. PMID: 9219317 Review.
-
Meloxicam: selective COX-2 inhibition in clinical practice.Semin Arthritis Rheum. 1997 Jun;26(6 Suppl 1):21-7. doi: 10.1016/s0049-0172(97)80049-2. Semin Arthritis Rheum. 1997. PMID: 9219316 Review.
Cited by
-
Ibuprofen: pharmacology, efficacy and safety.Inflammopharmacology. 2009 Dec;17(6):275-342. doi: 10.1007/s10787-009-0016-x. Epub 2009 Nov 21. Inflammopharmacology. 2009. PMID: 19949916 Review.
-
Synthesis, in-vitro inhibition of cyclooxygenases and in silico studies of new isoxazole derivatives.Front Chem. 2023 Sep 6;11:1222047. doi: 10.3389/fchem.2023.1222047. eCollection 2023. Front Chem. 2023. PMID: 37744065 Free PMC article.
-
PharmGKB summary: ibuprofen pathways.Pharmacogenet Genomics. 2015 Feb;25(2):96-106. doi: 10.1097/FPC.0000000000000113. Pharmacogenet Genomics. 2015. PMID: 25502615 Free PMC article. No abstract available.
-
Subcutaneous meloxicam suspension pharmacokinetics in mice and dose considerations for postoperative analgesia.J Vet Pharmacol Ther. 2016 Aug;39(4):356-62. doi: 10.1111/jvp.12297. Epub 2016 Feb 20. J Vet Pharmacol Ther. 2016. PMID: 26896236 Free PMC article.
-
Observational study of upper gastrointestinal haemorrhage in elderly patients given selective cyclo-oxygenase-2 inhibitors or conventional non-steroidal anti-inflammatory drugs.BMJ. 2002 Sep 21;325(7365):624. doi: 10.1136/bmj.325.7365.624. BMJ. 2002. PMID: 12242172 Free PMC article.
References
-
- Vane JR. Inhibition of prostaglandins as a mechanism of action for aspirin-like drugs. Nature New Biol. 1971;231:232–235. - PubMed
-
- Dubois RN, Abramson SB, Crofford L, et al. Cyclooxygenase in biology and disease. FASEB J. 1998;12:1063–1073. - PubMed
-
- Vane JR, Bakhle YS, Botting RM. Cyclooxygenases 1 and 2. Annu Rev Pharmacol Toxicol. 1998;38:97–120. - PubMed
-
- Meade EA, Smith WL, DeWitt DL. Differential inhibition of prostaglandin endoperoxide synthase (cyclooxygenase) isoenzymes by aspirin and other non-steroidal anti inflammatory drugs. J Biol Chem. 1993;268:6610–6614. - PubMed
-
- Battistini B, Botting R, Bakhle YS. Cox-1 and Cox-2: Towards the development of more selective NSAIDs. Drug News Perspectives. 1994;7:501–512.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
