

The declining comprehensiveness of primary care
- PMID: 11876170
- PMCID: PMC99351
The declining comprehensiveness of primary care
Abstract
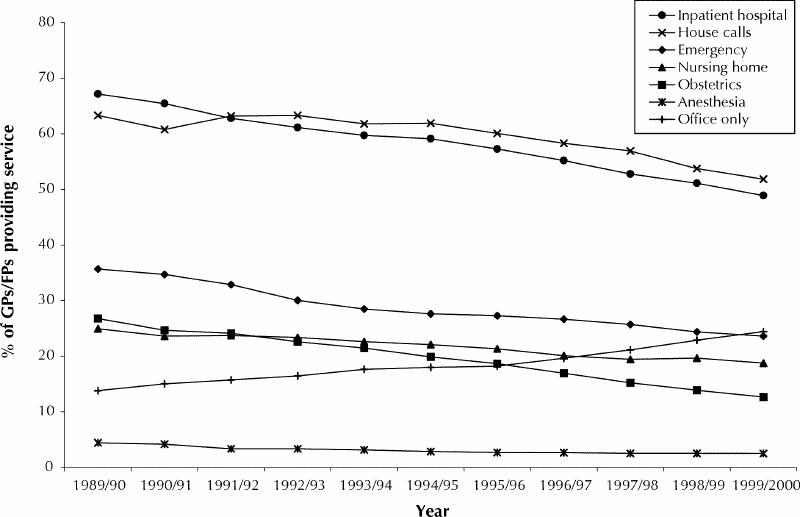
Background: Recent studies suggest that comprehensiveness of primary care has declined steadily over the past decade. This study tracks the participation rates of general practitioners and family physicians in 6 nonoffice settings across Ontario and examines among which types of physicians this decline in comprehensiveness has occurred.
Methods: Billing (claims) records were used to determine the proportions of fee-for-service general practitioners and family physicians who provided emergency, inpatient, nursing home, house call, anesthesia or obstetrical services from 1989/90 to 1999/2000. "Office-only" physicians were those who worked in none of these nonoffice settings. The relation of various physician characteristics to comprehensiveness of care was tested with multivariate analysis for 1999/2000.
Results: The proportion of "office-only" general practitioners and family physicians rose from 14% in 1989/90 to 24% in 1999/2000 (p < 0.001). Significant increases in this proportion were noted among general practitioners and family physicians of all ages, both sexes and all practice locations. In 1999/2000, recent graduates (who had completed medical school within the past 7 years) had higher participation rates for emergency medicine (40% v. 5% for physicians aged 65 years and older); female physicians had higher participation rates for obstetrics (16% v. 11% for males); and older physicians had higher participation rates for nursing home visits and house calls (20% and 57% respectively v. 11% and 37% for recent graduates). However, "office-only" physicians were more likely to be female (odds ratio [OR] 2.65, 95% confidence interval [CI] 2.37-2.96), recent graduates (OR 1.35, 95% CI 1.15-1.60), aged 65 years and older (OR 1.45, 95% CI 1.20-1.75) or practising in a city with a medical school (OR 2.30, 95% CI 2.06-2.56) and were less likely to be rural physicians (OR 0.31, 95% CI 0.24-0.41) or certified in family medicine (OR 0.58, 95% CI 0.52-0.66).
Interpretation: There has been a decline in the provision of comprehensive care by general practitioners and family physicians in Ontario. The decline is evident across all age groups and for both male and female physicians. It is also evident in rural areas and in cities with and without medical schools.
Figures
References
-
- Kimball HR, Young PR. A statement on the generalist physician from the American Boards of Family Practice and Internal Medicine. JAMA 1994; 271 (4):315-6. - PubMed
-
- Starfield B. Primary care: concept, evaluation & policy. New York: Oxford University Press; 1992.
-
- Donaldson MS, Yordy KD, Lohr KN, Vanselow NA. Primary care: America's health in a new era. Washington: Institute of Medicine; 1996. p. 32. Available: www.books.nap.edu/catalog/5152.html (accessed 2001 Dec 10).
-
- Ontario College of Family Physicians. Family medicine in the 21st century: a prescription for excellence in health care. Toronto: The College; 1999. p. 13.
-
- Chan B. Supply of physicians' services in Ontario. Atlas reports: uses of health services. Toronto: Institute for Clinical Evaluative Sciences; 1999.
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous