

Role of somatostatin-14 and its analogues in the management of gastrointestinal fistulae: clinical data
- PMID: 11878789
- PMCID: PMC1766896
- DOI: 10.1136/gut.49.suppl_4.iv11
Role of somatostatin-14 and its analogues in the management of gastrointestinal fistulae: clinical data
Abstract
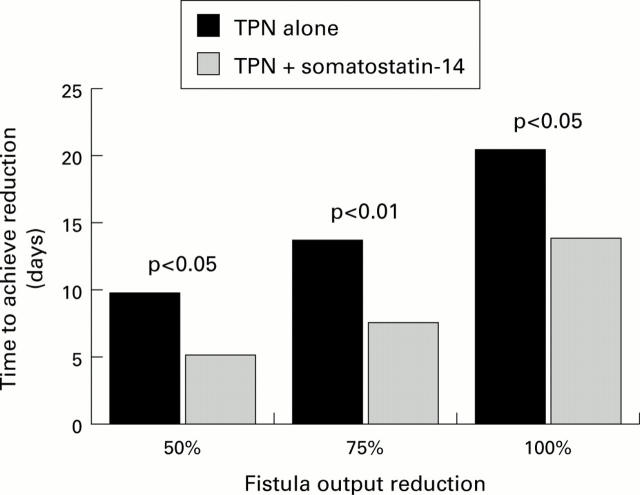
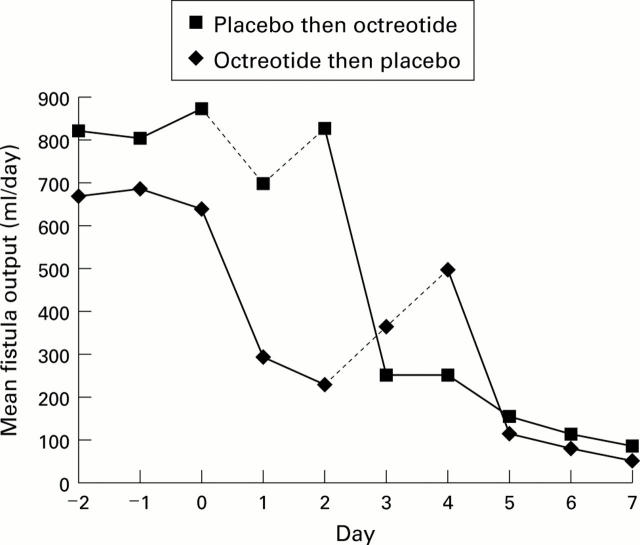
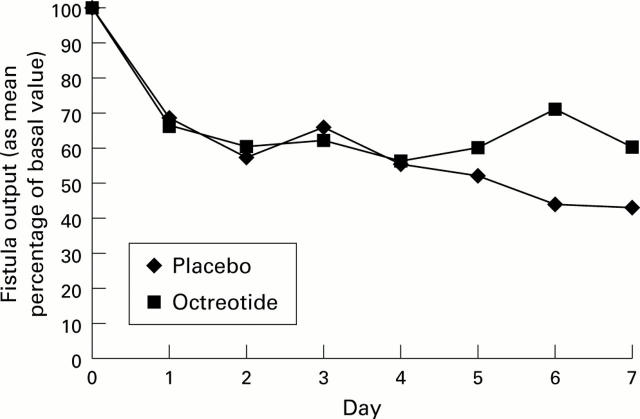
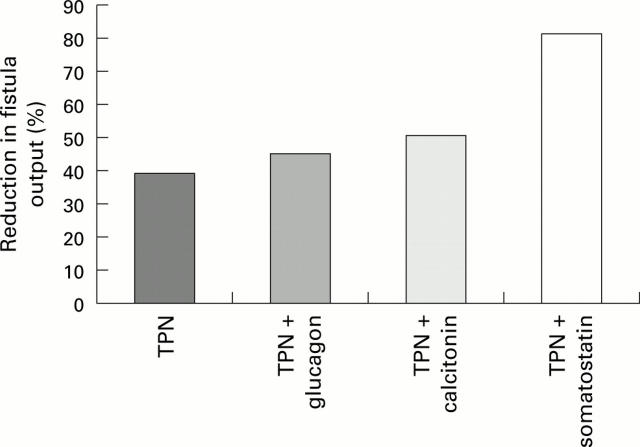
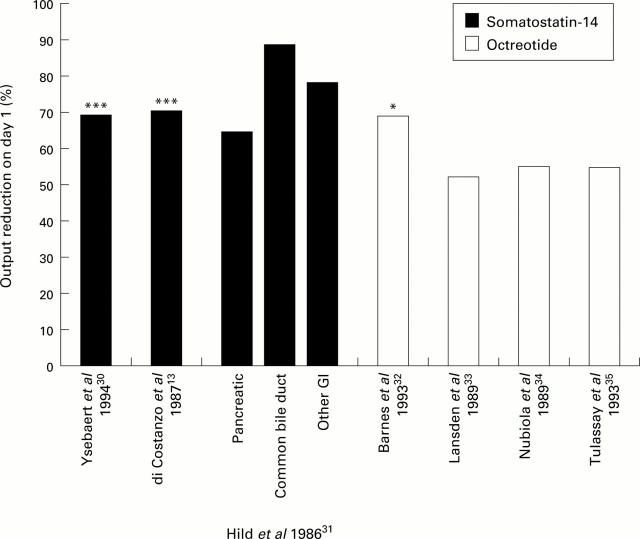
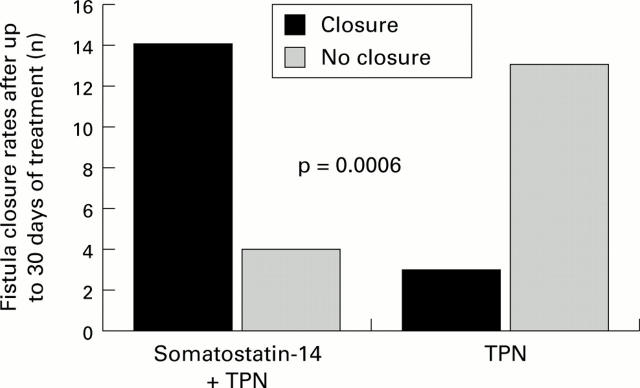
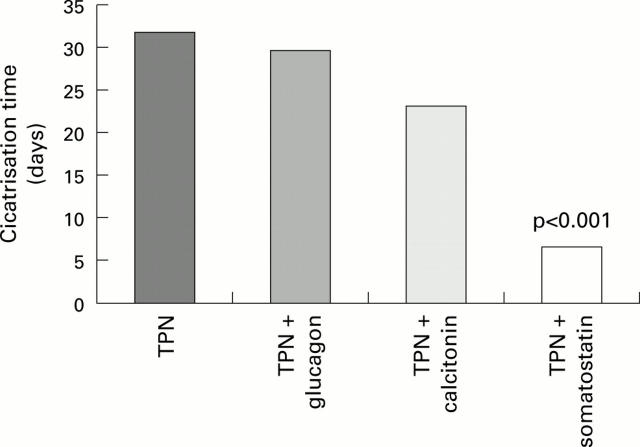
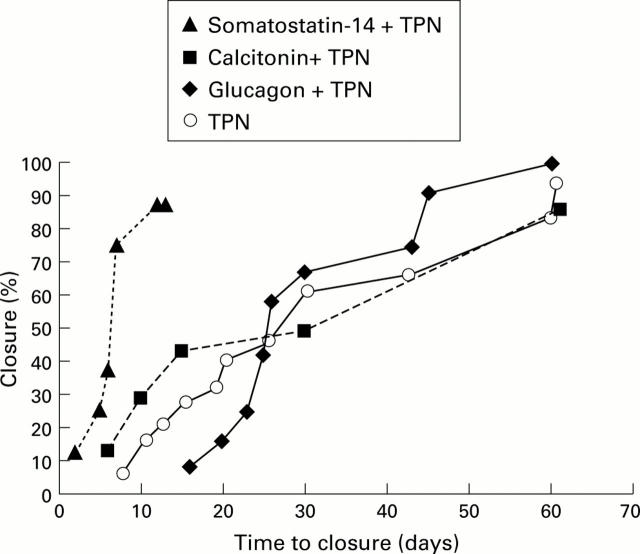
Somatostatin-14 and its analogue octreotide both exert inhibitory effects on gastrointestinal secretions and may therefore be beneficial in the treatment of gastrointestinal fistulae. There are no studies that have compared these two drugs directly and hence this paper aims to review studies that are available for each drug. There are only six controlled studies that have examined the effects of somatostatin-14 and octreotide on fistula output reduction, three for each drug. All studies compared conservative therapy and the drug in combination with conservative therapy. Of the somatostatin-14 studies, two showed a significant effect on output (p<0.05) and the other demonstrated an output reduction on day 1 that was twice that in the control group (NS). Of the octreotide studies, one showed a significant effect (p<0.01) and the other two showed no effect of the drug on output. No study with either drug has demonstrated an increase in the number of patients that have achieved closure. However, a positive effect on the time to achieve closure has been found. Of the five controlled studies with somatostatin-14, all showed a significant reduction in time to closure. Of the two controlled studies with octreotide, one showed a significant reduction (p=0.002) and the other showed no difference. Due to the limited number of trials, a definitive evaluation of the efficacies of somatostatin-14 and octreotide in the treatment of gastrointestinal fistulae is not possible. However, currently available information seems to suggest a considerable benefit of somatostatin-14 when administered in association with standard conservative treatment, but this needs to be confirmed in a large prospective controlled study.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous