

Laparoscopic repair for perforated peptic ulcer: a randomized controlled trial
- PMID: 11882751
- PMCID: PMC1422436
- DOI: 10.1097/00000658-200203000-00001
Laparoscopic repair for perforated peptic ulcer: a randomized controlled trial
Abstract
Objective: To compare the results of open versus laparoscopic repair for perforated peptic ulcers.
Summary background data: Omental patch repair with peritoneal lavage is the mainstay of treatment for perforated peptic ulcers in many institutions. Laparoscopic repair has been used to treat perforated peptic ulcers since 1990, but few randomized studies have been carried out to compare open versus laparoscopic procedures.
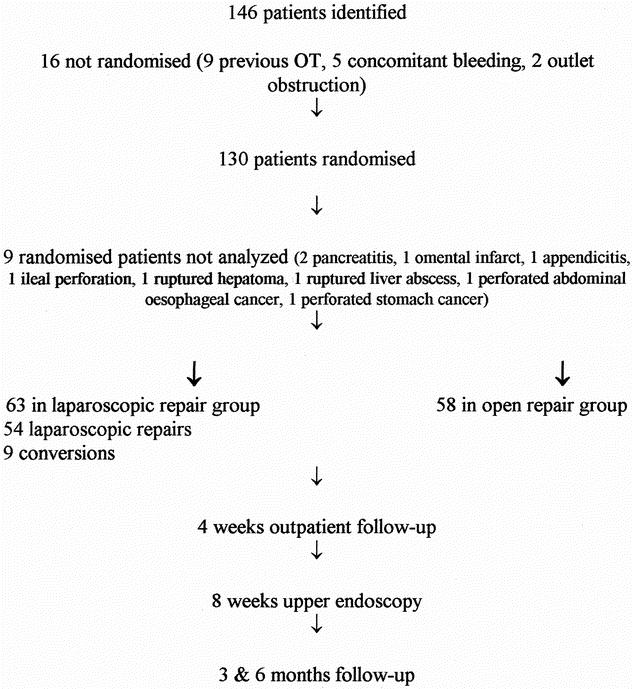
Methods: From January 1994 to June 1997, 130 patients with a clinical diagnosis of perforated peptic ulcer were randomly assigned to undergo either open or laparoscopic omental patch repair. Patients were excluded for a history of upper abdominal surgery, concomitant evidence of bleeding from the ulcer, or gastric outlet obstruction. Patients with clinically sealed-off perforations without signs of peritonitis or sepsis were treated without surgery. Laparoscopic repair would be converted to an open procedure for technical difficulties, nonjuxtapyloric gastric ulcers, or perforations larger than 10 mm. A Gastrografin meal was performed 48 to 72 hours after surgery to document sealing of the perforation. The primary end-point was perioperative parenteral analgesic requirement. Secondary endpoints were operative time, postoperative pain score, length of postoperative hospital stay, complications and deaths, and the date of return to normal daily activities.
Results: Nine patients with a surgical diagnosis other than perforated peptic ulcer were excluded; 121 patients entered the final analysis. There were 98 male and 23 female patients recruited, ages 16 to 89 years. The two groups were comparable in age, sex, site and size of perforations, and American Society of Anesthesiology classification. There were nine conversions in the laparoscopic group. After surgery, patients in the laparoscopic group required significantly less parenteral analgesics than those who underwent open repair, and the visual analog pain scores in days 1 and 3 after surgery were significantly lower in the laparoscopic group as well. Laparoscopic repair required significantly less time to complete than open repair. The median postoperative stay was 6 days in the laparoscopic group versus 7 days in the open group. There were fewer chest infections in the laparoscopic group. There were two intraabdominal collections in the laparoscopic group. One patient in the laparoscopic group and three patients in the open group died after surgery.
Conclusions: Laparoscopic repair of perforated peptic ulcer is a safe and reliable procedure. It was associated with a shorter operating time, less postoperative pain, reduced chest complications, a shorter postoperative hospital stay, and earlier return to normal daily activities than the conventional open repair.
Comment in
-
Laparoscopic repair for perforated peptic ulcer.Ann Surg. 2002 Mar;235(3):320-1. doi: 10.1097/00000658-200203000-00002. Ann Surg. 2002. PMID: 11882752 Free PMC article. No abstract available.
References
-
- Koo J, Ngan YK, Lam SK. Trends in hospital admissions, perforation and mortality of peptic ulcer in Hong Kong from 1970 to 1980. Gastroenterology 1983; 84: 1558–1562. - PubMed
-
- Alagaratnam TT, Wong J. No decrease in duodenal ulcer surgery after cimetidine in Hong Kong. J Clin Gastroenterol 1988; 10: 25–27. - PubMed
-
- Crofts TJ, Park KGM, Steel RJC, et al. A randomized trial of non-operative treatment for perforated peptic ulcer. N Engl J Med 1989; 320: 970–973. - PubMed
-
- Gunshefski L, Flancbaum L, Brolin RE, Frankei A. Changing patterns in perforated peptic ulcer disease. Am Surg 1990; 56: 270–274. - PubMed
-
- Cocks JR. Perforated peptic ulcer: the changing scene. Dig Dis 1992; 10: 10–16. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
