

Repair of groin hernia with synthetic mesh: meta-analysis of randomized controlled trials
- PMID: 11882753
- PMCID: PMC1422456
- DOI: 10.1097/00000658-200203000-00003
Repair of groin hernia with synthetic mesh: meta-analysis of randomized controlled trials
Abstract
Objective: To measure the effects of laparoscopic and open placement of synthetic mesh on recurrence and persisting pain following groin hernia repair.
Summary background data: Synthetic mesh techniques are claimed to reduce the risk of recurrence but there are concerns about costs and possible long-term complications, particularly pain.
Methods: Electronic databases were searched and experts consulted to identify randomized or quasi-randomized trials that compared mesh with non-mesh methods, or laparoscopic with open mesh placement. Individual patient data were sought for each trial. Aggregated data were used where individual patient data were not available. Meta-analyses of hernia recurrence and persisting pain were based on intention to treat.
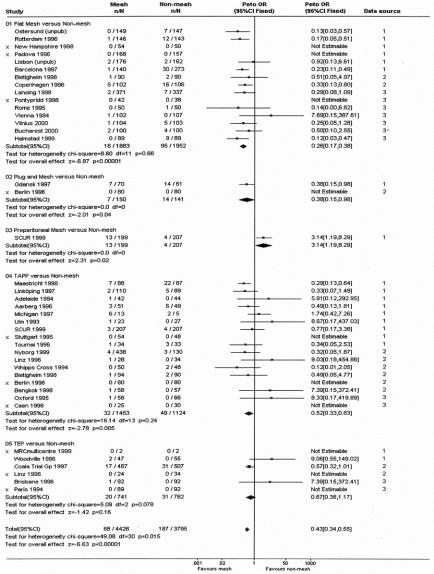
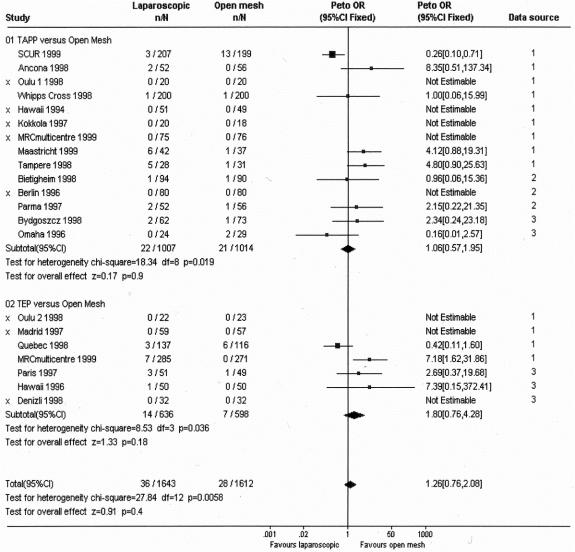
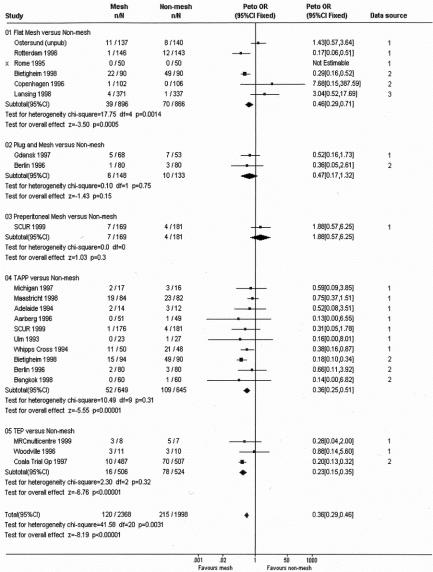
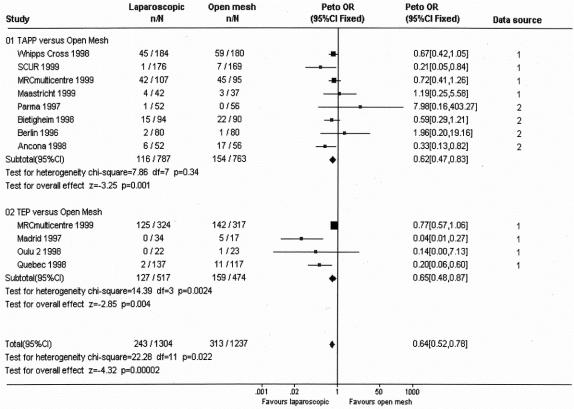
Results: There were 62 relevant comparisons in 58 trials. These included 11,174 participants: individual patient data were available for 6,901 patients, supplementary aggregated data for 2,390 patients, and published data for 1883 patients. Recurrence and persisting pain were less after mesh repair (overall recurrences: 88 in 4,426 vs. 187 in 3,795; OR 0.43, 95% CI 0.34-0.55; P <.001) (overall persistent pain: 120 in 2,368 vs. 215 in 1,998; OR 0.36, 95% CI 0.29-0.46; P <.001), regardless of the non-mesh comparator. Whereas the reduction in recurrence was similar after laparoscopic and open mesh placement (OR 1.26, 95% CI 0.76-2.08; P =.36), persistent pain was less common after laparoscopic than open mesh placement (OR 0.64; 95% CI 0.52-0.78; P <.001).
Conclusions: The use of synthetic mesh substantially reduces the risk of hernia recurrence irrespective of placement method. Mesh repair appears to reduce the chance of persisting pain rather than increase it.
Figures
References
-
- Liem MSL, van Vroonhoven TJMV. Laparoscopic inguinal hernia repair. Br J Surg 1996; 83: 1197–204. - PubMed
-
- EU Hernia Trialists Collaboration. Mesh compared with non-mesh methods of open groin hernia repair: systematic review of randomized controlled trials. Br J Surg 2000; 87: 854–9. - PubMed
-
- EU Hernia Trialists Collaboration. Laparoscopic compared with open methods of groin hernia repair: systematic review of randomized controlled trials. Br J Surg 2000; 87: 860–7. - PubMed
-
- EU Hernia Trialists Collaboration. Overview of randomised trials of inguinal hernia repair - A European Concerted Action. Surg Endosc 1999; 13: 1030–1. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
