

Hepatic abscess in patients with chronic granulomatous disease
- PMID: 11882760
- PMCID: PMC1422444
- DOI: 10.1097/00000658-200203000-00010
Hepatic abscess in patients with chronic granulomatous disease
Abstract
Objective: To evaluate the clinical presentation, diagnostic procedures, and surgical management of hepatic abscesses in patients with chronic granulomatous disease (CGD).
Summary background data: Chronic granulomatous disease is a rare inherited primary immunodeficiency in which phagocytes cannot destroy catalase-positive bacteria and fungi. Defects in the phagocytic cells' respiratory burst lead to life-threatening infections, including hepatic abscess. These abscesses are recurrent and often multiple and are treated differently from bacterial abscesses in patients without CGD.
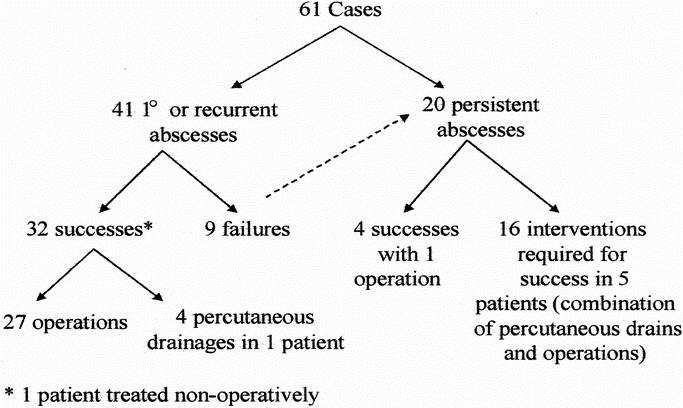
Methods: Between 1980 and 2000, 61 cases of hepatic abscess in 22 patients with CGD were treated at the National Institutes of Health. Clinicopathologic features were investigated by retrospective review of the medical records, radiographs, and histopathology.
Results: Twelve of the 61 cases were primary hepatic abscesses. Twenty-nine of the cases were recurrent hepatic abscesses, and 20 cases were persistent hepatic abscesses. The median age at the time of initial hepatic abscess presentation was 14 years. Subjective fever was the most frequent presenting symptom, and the erythrocyte sedimentation rate was elevated in 98% of cases. Fifty-two cases were managed surgically and eight cases were managed with percutaneous drainage. One patient refused surgery. The surgical complication rate was 56%; however, there were no deaths directly related to the hepatic abscesses. Staphylococcus aureus was the most frequent organism identified in culture (88% of positive cultures). Aggressive surgery and antibiotics ultimately resulted in successful treatment of all patients.
Conclusions: Hepatic abscesses occurring in patients with CGD represent a difficult diagnostic and treatment challenge. Early excision and treatment with antibiotics directed against S. aureus is necessary. General surgeons should be aware of this rare immunodeficiency and should aggressively manage hepatic abscesses in these patients.
Figures
References
-
- Segal BH, Leto TL, Gallin JI, et al. Genetic, biochemical, and clinical features of chronic granulomatous disease. Medicine 2000; 79 (3): 170–200. - PubMed
-
- Lekstrom-Himes JA, Gallin JI. Immunodeficiency diseases caused by defects in phagocytes. N Engl J Med 2000; 343 (23): 1703–1714. - PubMed
-
- Winkelstein JA, Marino MC, Johnston RB, et al. Chronic granulomatous disease. Report on a national registry of 368 patients. Medicine 2000; 79 (3): 155–169. - PubMed
-
- Roback SA, Weintraub WH, Good RA, et al. Chronic granulomatous disease of childhood: surgical considerations. J Pediatr Surg 1971; 6: 601–611. - PubMed
-
- Mulholland MW, DeLaney JP, Simmons RL. Gastrointestinal complications of chronic granulomatous disease: surgical implications. Surgery 1983; 94: 569–575. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
