

Diagnostic accuracy of forceps biopsy versus polypectomy for gastric polyps: a prospective multicentre study
- PMID: 11889063
- PMCID: PMC1773183
- DOI: 10.1136/gut.50.4.465
Diagnostic accuracy of forceps biopsy versus polypectomy for gastric polyps: a prospective multicentre study
Abstract
Aims: To determine whether an adequate histological diagnosis of gastric polyps can be attained on the basis of forceps biopsy.
Patients and methods: In a prospective multicentre study, 194 patients with 222 endoscopically removable gastric polyps (>or=5 mm) underwent forceps biopsy and complete polypectomy. Patients with fundic gland polyps and polyposis syndrome were not included. Specimens were evaluated by primary and reference pathologists, and the complication rate of gastric polypectomy was also determined.
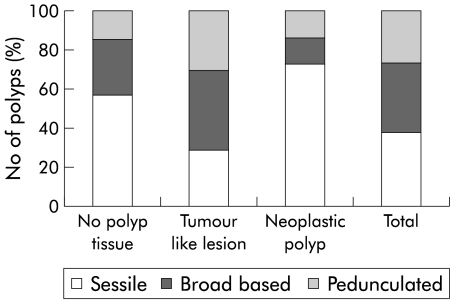
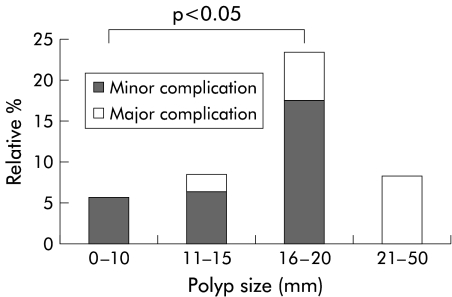
Results: Of the 222 polyps, histological examination of the polypectomy specimens revealed tumour-like lesions in 77% (10% focal foveolar hyperplasia, 59% hyperplastic polyps, 4% inflammatory fibroid polyps, 4% other polyps) and neoplasia in 19% (10% tubular adenoma, 2% tubulovillous adenoma, 1% high grade intraepithelial neoplasia, 6% adenocarcinoma). When biopsy results were compared, complete agreement was found in 124 cases (55.8%) and, in an additional 77 cases (34.7%), the clinically important differentiation between tumour-like lesions and neoplasia was possible. However, relevant differences were found by the reference pathologist in six cases (2.7%), the most common reason being failure of biopsy to reveal foci of carcinoma in hyperplastic polyps. Bleeding was observed after polypectomy in 16 patients (7.2%), in 15 of whom it was managed conservatively.
Conclusions: We recommend complete removal by an experienced endoscopist of all epithelial gastric polyps larger than 5 mm after thorough individualised risk-benefit analysis.
Figures
References
-
- Seifert E, Elster K. Gastric polypectomy. Am J Gastroenterol 1975;63:451–6. - PubMed
-
- Ottenjann R, Kunert H, Seib HJ. Is gastroscopic polypectomy a diagnostic necessity? Results of a prospective study. Dtsch Med Wochenschr 1984;109:443–5. - PubMed
-
- Chua CL. Gastric polyps: the case for polypectomy and endoscopic surveillance. J R Coll Surg Edinb 1990;35:163–5. - PubMed
-
- Ginsberg GG, Al-Kawas FH, Fleischer DE, et al. Gastric polyps: relationship of size and histology to cancer risk. Am J Gastroenterol 1996;91:714–17. - PubMed
-
- Jass JR, Sobin LH, Watanabe H. The World Health Organization's histologic classification of gastrointestinal tumors. A commentary on the second edition. Cancer 1990;66:2162–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical