

Frailty, fitness and late-life mortality in relation to chronological and biological age
- PMID: 11897015
- PMCID: PMC88955
- DOI: 10.1186/1471-2318-2-1
Frailty, fitness and late-life mortality in relation to chronological and biological age
Abstract
Background: People age at remarkably different rates, but how to estimate trajectories of senescence is controversial.
Methods: In a secondary analysis of a representative cohort of Canadians aged 65 and over (n = 2914) we estimated a frailty index based on the proportion of 20 deficits observed in a structured clinical examination. The construct validity of the index was examined through its relationship to chronological age (CA). The criterion validity was examined in its ability to predict mortality, and in relation to other predictions about aging. From the frailty index, relative (to CA) fitness and frailty were estimated, as was an individual's biological age.
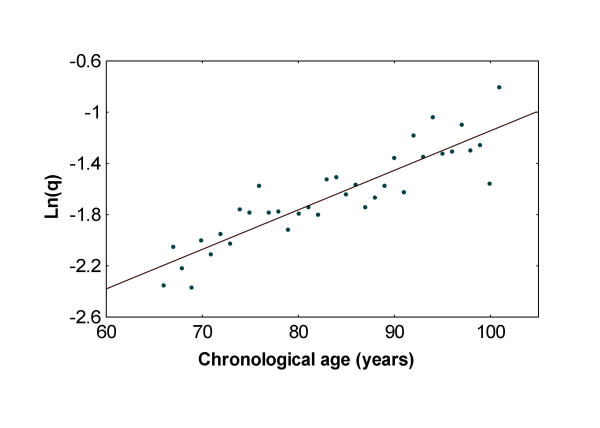
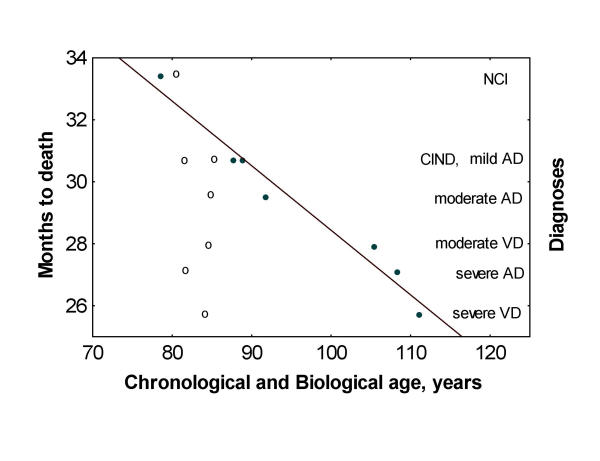
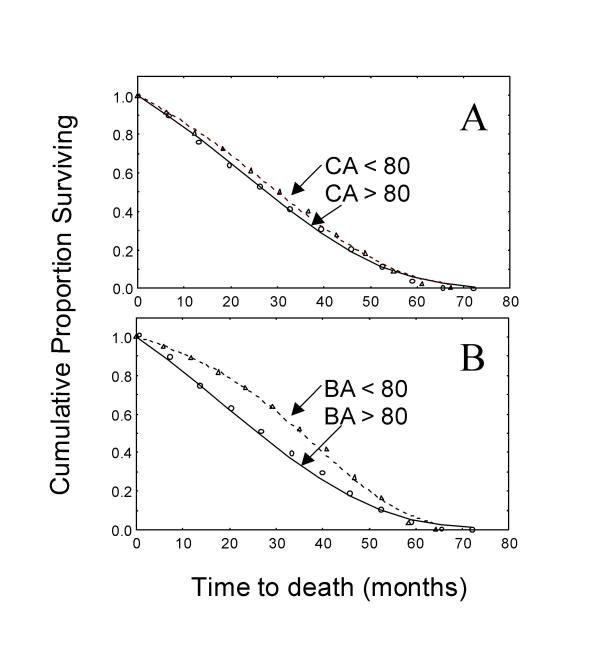
Results: The average value of the frailty index increased with age in a log-linear relationship (r = 0.91; p < 0.001). In a Cox regression analysis, biological age was significantly more highly associated with death than chronological age. The average increase in the frailty index (i.e. the average accumulation of deficits) amongst those with no cognitive impairment was 3 per cent per year.
Conclusions: The frailty index is a sensitive predictor of survival. As the index includes items not traditionally related to adverse health outcomes, the finding is compatible with a view of frailty as the failure to integrate the complex responses required to maintain function.
Figures
References
-
- Reisberg B, Ferris SH, de-Leon MJ, Crook T. The Global Deterioration Scale for assessment of primary degenerative dementia. Am J of Psych. 1982;139:1136–1139. - PubMed
-
- Hébert R, Brayne C, Spiegelhalter D. Factors associated with functional decline and improvement in a very elderly community-dwelling population. AMJE. 1999;150:501–510. - PubMed
-
- Seeman TE, Berkman LF, Charpentier PA, Blazer DG, Albert MS, Tinetti ME. Behavioural and psychosocial predictors of physical performance: MacArthur studies of successful aging. J Gerontol A Biol Sci Med Sci. 1995;50:M177–M183. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
