

Case Reports
Treatment of iatrogenic internal carotid artery laceration and carotid cavernous fistula with endovascular stent-graft placement
Affiliations
- PMID: 11901015
- PMCID: PMC7975307
Item in Clipboard
Case Reports
Treatment of iatrogenic internal carotid artery laceration and carotid cavernous fistula with endovascular stent-graft placement
AJNR Am J Neuroradiol.
2002 Mar.
Abstract
The risk of fatal injury of the internal carotid artery (ICA) and surrounding anatomy during transsphenoidal surgery for pituitary adenoma is the most severe potential complication associated with this particular approach. We present a case in which iatrogenic injury to a patient's ICA and resultant carotid cavernous fistula and massive hemorrhage was successfully managed with the emergency placement of an endovascular stent-graft. Both findings in the relevant literature and practical considerations concerning both stent-grafts and other more commonly used options for the treatment of iatrogenic ICA injury are discussed.
Figures
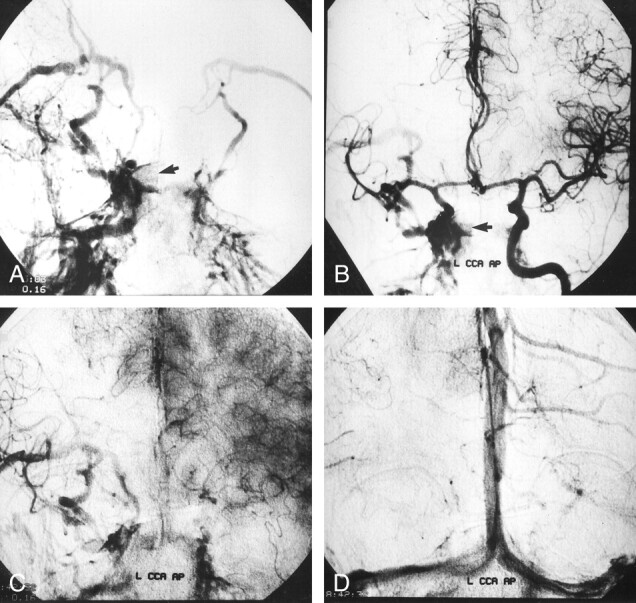
Angiograms obtained with external compression of the right CCA in a 58- year-old woman with iatrogenic right ICA injury associated with TSS. A and B, Right (A) and left (B) CCA angiograms, anteroposterior projections, reveal contrast material extravasation within the sphenoid sinus (arrow) and show a high-flow CCF draining toward the superior ophthalmic vein, pterygoid plexus, and petrosal sinuses. C and D, Left CCA angiograms reveal prominent circulation delays in the capillary (C) and venous (D) phases on the right side in comparison with the left side.
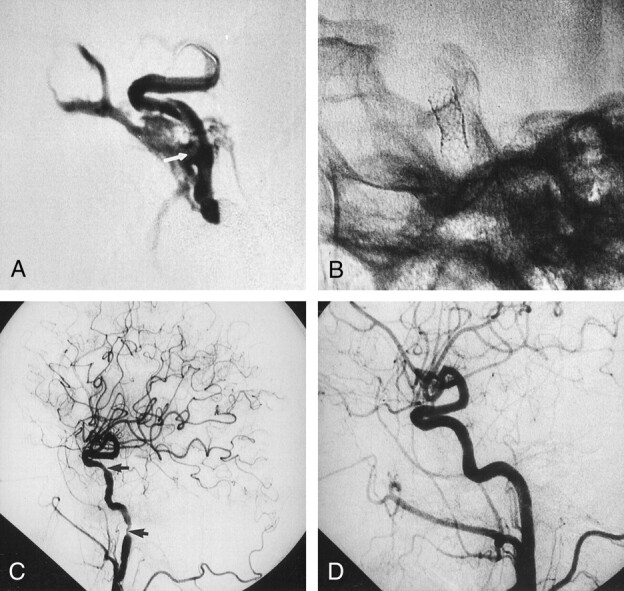
Coronary stent-graft placement to treat an iatrogenic ICA injury. A, Contrast material injection from the guiding catheter reveals the lacerated segment of the right ICA (arrow) on this angiogram. Note that the stent-graft and microguidewire are in the ICA lumen during the injection. B, Fluoroscopic image obtained after removal of the microballoon and microguidewire shows the expanded stent-graft in the lacerated ICA. C, Postprocedural right CCA angiogram obtained after deployment of stent-graft reveals cessation of contrast material extravasation and closure of the CCF. Note the focal transient spasm distal to the stent-graft and at the subpetrous portion of cervical ICA (arrows). D, Right CCA angiogram obtained 3 mo after the procedure demonstrates patency of the ICA, with no contour irregularity.
References
-
- Hardy J, McCutcheon IE. Pituitary microadenomas.In: Apuzzo MLJ, ed. Brain Surgery: Complications Avoidance and Management. New York, NY: Churchill Livingstone;1992;33–122
-
- Ciric I, Ragin A, Baumgartner C, Pierce D. Complications of transsphenoidal surgery: results of a national survey, review of the literature, and personal experience. Neurosurgery 1997;40:225–236 - PubMed
-
- Lee KJ. The sublabial transseptal transsphenoidal approach to the hypophysis. Laryngoscope 1978;88:1–65 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous