

Using disease risk estimates to guide risk factor interventions: field test of a patient workbook for self-assessing coronary risk
- PMID: 11906538
- PMCID: PMC5060131
- DOI: 10.1046/j.1369-6513.2002.00148.x
Using disease risk estimates to guide risk factor interventions: field test of a patient workbook for self-assessing coronary risk
Abstract
Objective: To assess the feasibility and acceptability of a patient workbook for self-assessing coronary risk.
Design: Pilot study, with post-study physician and patient interviews.
Setting and subjects: Twenty southern Ontario family doctors and 40 patients for whom they would have used the workbook under normal practice conditions.
Interventions: The study involved convening two sequential groups of family physicians: the first (n=10) attended focus group meetings to help develop the workbook (using algorithms from the Framingham Heart Study); the second (n=20) used the workbook in practice with 40 patients. Follow-up interviews were by interviewer-administered questionnaire.
Main outcomes measures: Physicians' and patients' opinions of the workbook's format, content, helpfulness, feasibility, and potential for broad application, as well as patients' perceived 10-year risk of a coronary event measured before and after using the workbook.
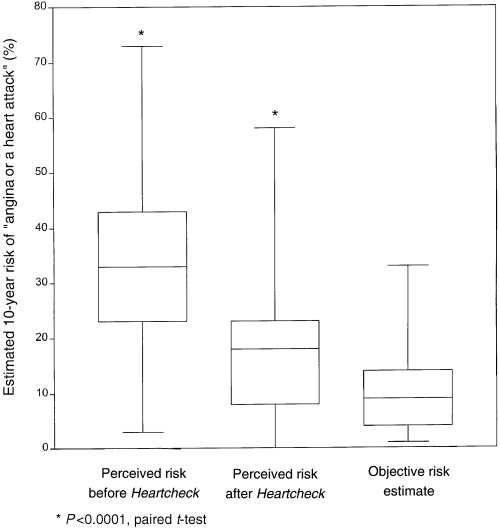
Results: It took an average of 18 minutes of physician time to use the workbook: roughly 7 minutes to introduce it to patients, and about 11 minutes to discuss the results. Assessments of the workbook were generally favourable. Most patients were able to complete it on their own (78%), felt they had learned something (80%) and were willing to recommend it to someone else (98%). Similarly, 19 of 20 physicians found it helpful and would use it in practice with an average of 18% of their patients (range: 1-80%). The workbook helped to correct misperceptions patients had about their personal risk of a coronary event over the next 10 years (pre-workbook (mean (SD) %): 35.2 (16.9) vs. post-workbook: 17.3 (13.5), P < 0.0001; estimate according to algorithm: 10.6 (7.6)).
Conclusions: Given a simple tool, patients can and will assess their own risk of CHD. Such tools could help inform otherwise healthy individuals that their risk is increased, allowing them to make more informed decisions about their behaviours and treatment.
Figures
References
-
- Anderson KM, Wilson PWF, Odell PM, Kannel WB. An updated coronary risk profile: a statement for health professionals. Circulation, 1991; 83 : 356–362. - PubMed
-
- Wood D, De Backer G, Faergeman O, Graham I, Mancia G, Pyorala K. Prevention of coronary heart disease in clinical practice: recommendations of the Second Joint Task Force of European and other Societies on Coronary Prevention. Atherosclerosis, 1998; 140 : 199–270. - PubMed
-
- Grundy SM, Balady GJ, Criqui MH et al. Primary prevention of coronary heart disease: guidance from Framingham: a statement for healthcare professionals from the AHA Task Force on Risk Reduction. American Heart Association. Circulation, 1998; 97 : 1876–1887. - PubMed
-
- Brett AS. Ethical issues in risk factor modification. American Journal of Medicine, 1984; 76 : 557–561. - PubMed
-
- Farrow L, Wartman SA, Brock DW. Science, ethics, and the making of clinical decisions: implications for risk factor modification. Journal of the American Medical Association, 1988; 259 : 3161–3167. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
