

Rates of circumferential resection margin involvement vary between surgeons and predict outcomes in rectal cancer surgery
- PMID: 11923599
- PMCID: PMC1422458
- DOI: 10.1097/00000658-200204000-00001
Rates of circumferential resection margin involvement vary between surgeons and predict outcomes in rectal cancer surgery
Abstract
Objective: To analyze the potential variability in rates of circumferential resection margin (CRM) involvement between different surgeons and time periods and to determine the suitability of using CRM status as an immediate predictor of outcome after rectal cancer surgery.
Summary background data: After disease stage has been taken into account, survival in rectal cancer has been shown to be very variable between surgeons and institutions. One of the major factors influencing survival is local recurrence, and this in turn is strongly related to inadequate tumor excision, particularly at the CRM.
Methods: In a study involving 608 patients who underwent surgery for rectal cancer in Leeds during the 12-year period 1986 to 1997, the authors examined the role of CRM status as an immediate predictor of likely outcome, paying particular attention to its relationships with different surgeons and time periods.
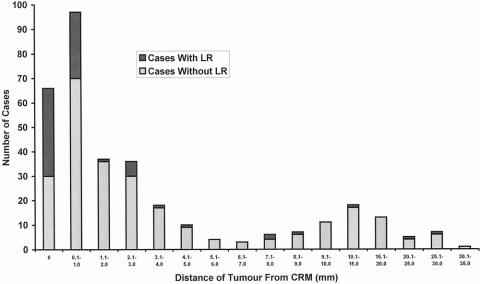
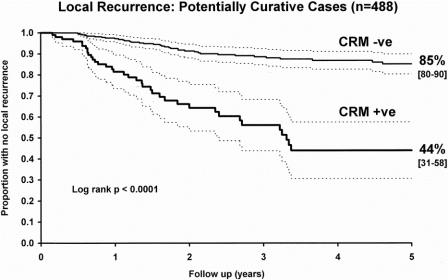
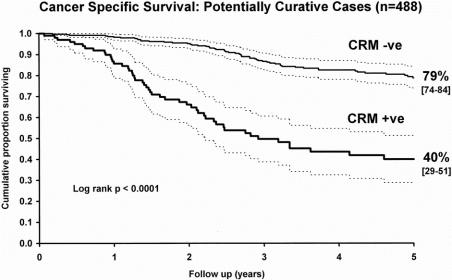
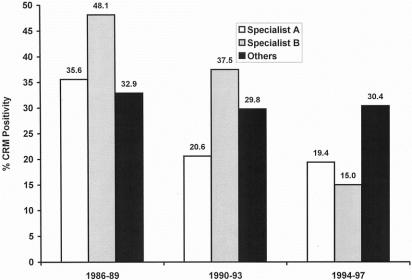
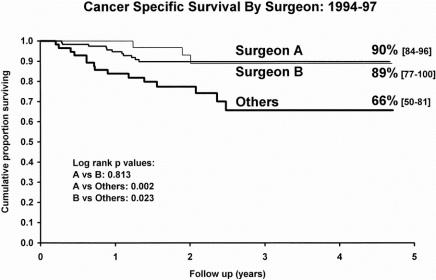
Results: Of 586 patients on whom full clinical follow-up was obtained, 165 (28.2%) had CRM involvement by carcinoma on pathologic examination. Up to the end of 1998, 105 (17.9%) patients had developed local recurrence. A significantly higher proportion (38.2%) of CRM-positive patients developed local recurrence than CRM-negative ones (10.0%). Kaplan-Meier survival analysis showed significant improvements in survival for CRM-negative patients over CRM-positive patients. Survival analysis in relation to two gastrointestinal surgeons and a group of other surgeons showed survival improvements that paralleled a reduction in the rates of CRM involvement for the two gastrointestinal surgeons during the period of the study. No improvement in survival or reduction in rates of CRM involvement was seen in the group of other surgeons.
Conclusions: These results show that CRM status may be used as an immediate predictor of survival after rectal cancer surgery and serves as a useful indicator of the quality of surgery. The frequency of CRM involvement can be used both for overall surgical audit and for monitoring the value of training programs in improving rectal surgery by individual surgeons. Its use in the current MRC CR07 study is valid and the best indicator of a requirement for further local therapy.
Figures
References
-
- Medical Research Council Rectal Cancer Working Party. Randomised trial of surgery alone versus surgery followed by radiotherapy for mobile cancer of the rectum. Lancet 1996; 348: 1610–1614. - PubMed
-
- The Norwegian Rectal Cancer Group. Total mesorectal excision (TME) in Norway: A national rectal cancer project. Dis Colon Rectum 1999; 42: A26.
-
- Heald RJ, Moran BJ, Ryall RD, et al. Rectal cancer: the Basingstoke experience of total mesorectal excision, 1978–1997. Arch Surg 1998; 133: 894–899. - PubMed
-
- Enker WE, Thaler HT, Cranor ML, et al. Total mesorectal excision in the operative treatment of carcinoma of the rectum. J Am Coll Surg 1995; 181: 335–346. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
