

Communicating accuracy of tests to general practitioners: a controlled study
- PMID: 11934776
- PMCID: PMC100792
- DOI: 10.1136/bmj.324.7341.824
Communicating accuracy of tests to general practitioners: a controlled study
Erratum in
- BMJ 2002 Jun 8;324(7350):1391
Abstract
Objective: To assess the extent to which different forms of summarising diagnostic test information influence general practitioners' ability to estimate disease probabilities.
Design: Controlled questionnaire study.
Setting: Three Swiss conferences in continuous medical education.
Participants: 263 general practitioners.
Intervention: Questionnaire with multiple choice questions about terms of test accuracy and a clinical vignette with the results of a diagnostic test described in three different ways (test result only, test result plus test sensitivity and specificity, test result plus the positive likelihood ratio presented in plain language).
Main outcome measures: Doctors' knowledge and application of terms of test accuracy and estimation of disease probability in the clinical vignette.
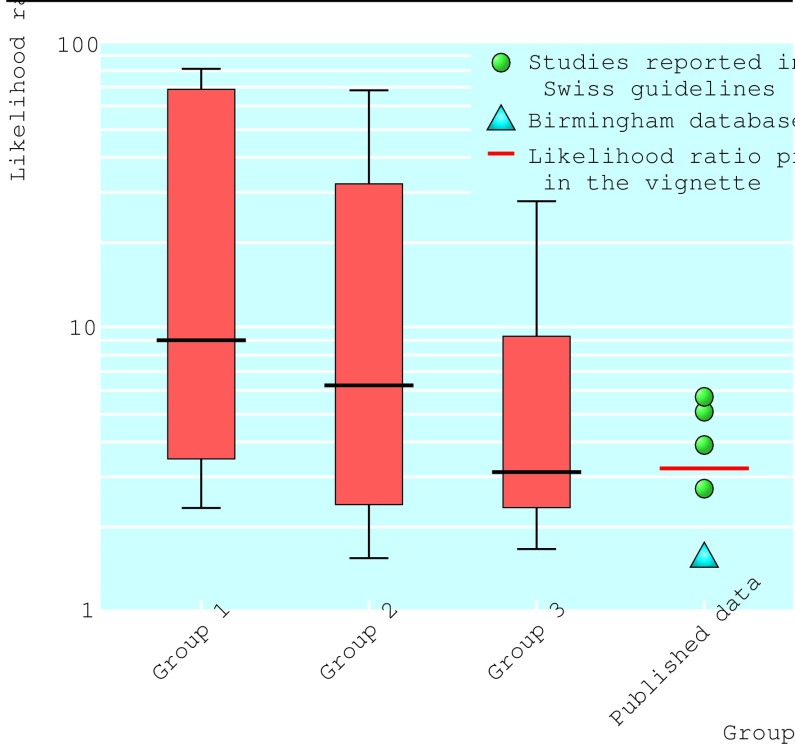
Results: The correct definitions for sensitivity and predictive value were chosen by 76% and 61% of the doctors respectively, but only 22% chose the correct answer for the post-test probability of a positive screening test. In the clinical vignette doctors given the test result only overestimated its diagnostic value (median attributed likelihood ratio (aLR)=9.0, against 2.54 reported in the literature). Providing the scan's sensitivity and specificity reduced the overestimation (median aLR=6.0) but to a lesser extent than simple wording of the likelihood ratio (median aLR=3.0).
Conclusion: Most general practitioners recognised the correct definitions for sensitivity and positive predictive value but did not apply them correctly. Conveying test accuracy information in simple, non-technical language improved their ability to estimate disease probabilities accurately.
Figures
References
-
- Eddy DM. Probabilistic reasoning in clinical medicine: problems and opportunities. In: Kahnemann D, Slovic P, Tversky A, editors. Judgement under uncertainty: heuristics and biases. Cambridge: Cambridge University Press; 1982. pp. 249–267.
-
- Hoffrage U, Lindsey S, Hertwig R, Gigerenzer G. Communicating statistical information. Science. 2000;290:2261. - PubMed
-
- Kahnemann D, Tversky A. Choices, values and frames. Cambridge: Cambridge University Press, Russel Sage Foundation; 2000.
-
- Clark TJ, Khan KS, Bakour SH, Gupta JK. Evaluation of outpatient hysteroscopy and ultrasonography in the diagnosis of endometrial disease. Obstet Gynecol (in press). - PubMed
-
- Bronz L, Dreher E, Almendral A, Studer A, Haller U. Abklärung von postmenopausalen Blutungen (PMBP) Schweizerische Aerztezeitung. 2000;81:1635–1646. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous