

Impact of reference-based pricing for angiotensin-converting enzyme inhibitors on drug utilization
- PMID: 11944760
- PMCID: PMC99452
Impact of reference-based pricing for angiotensin-converting enzyme inhibitors on drug utilization
Abstract
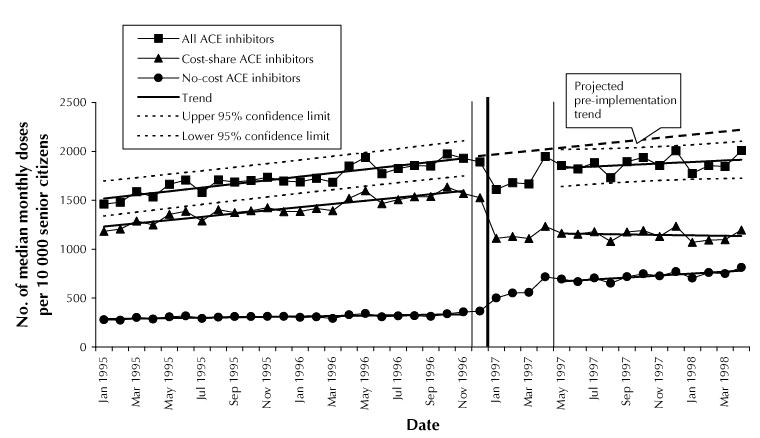
Background: Increasing copayments for higher-priced prescription medications has been suggested as a means to help finance drug coverage for elderly patients, but evaluations of the impact of such policies are rare. The objective of this study was to analyze the effect of reference-based pricing of angiotensin-converting enzyme (ACE) inhibitors on drug utilization, cost savings and potential substitution with other medication classes.
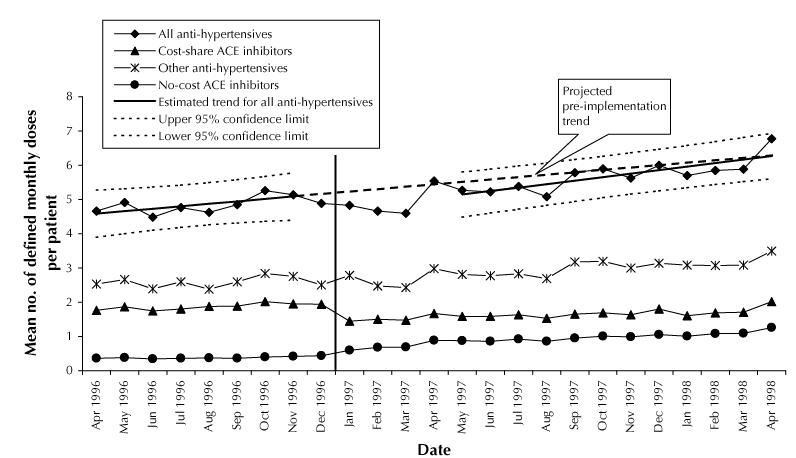
Methods: We analyzed 36 months of claims data from British Columbia for 2 years before and 1 year after implementation of reference-based pricing (in January 1997). The 119,074 patients were community-living Pharmacare beneficiaries 65 years of age or older who used ACE inhibitors during the study period. The main outcomes were changes over time in use of ACE inhibitors, use of antihypertensive drugs and expenditures for antihypertensive drugs, as well as predictors of medication switching related to reference-based pricing.
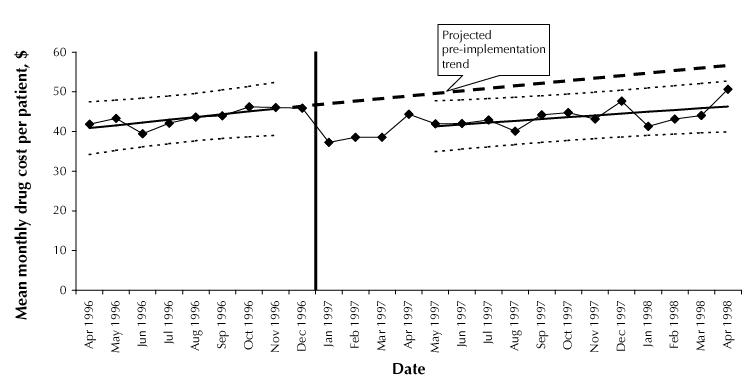
Results: We observed a sharp decline (29%) in the use of higher-priced cost-shared ACE inhibitors immediately after implementation of the policy (p < 0.001). After a transition period, the post-implementation utilization rate for all ACE inhibitors was 11% lower than projected from pre-implementation data. However, overall utilization of antihypertensives was unchanged (p = 0.40). The policy saved $6.7 million in pharmaceutical expenditures during its first 12 months. Patients with heart failure or diabetes mellitus who were taking a cost-shared ACE inhibitor were more likely to remain on the same medication after implementation of reference-based pricing (OR 1.12 [95% confidence interval, CI, 1.06-1.19] and 1.28 [95% CI 1.20-1.36] respectively). Patients with low-income status were more likely than those with high-income status to stop all antihypertensive therapy (OR 1.65 [95% CI 1.43-1.89]), which reflects a general trend toward discontinuation of therapy among these patients even before implementation of reference-based pricing.
Interpretation: Reference-based pricing in British Columbia achieved a sustained reduction in drug expenditures, and no changes in overall use of antihypertensive therapy were observed. Further research is needed on the overall health and economic effects of such policies.
Figures
Comment in
-
Why is calling an ACE an ACE so controversial? Evaluating reference-based pricing in British Columbia.CMAJ. 2002 Mar 19;166(6):763-4. CMAJ. 2002. PMID: 11944763 Free PMC article. No abstract available.
References
-
- Canadian Institute for Health Information. Spending on drugs outpaces other health care spending, reports CIHI [press release]. Ottawa: The Institute; 2001 Mar 14. Available: www.cihi.ca/medrls/14mar2001.shtml (accessed 2001 Jan 9).
-
- Iglehart JK. The American health care system. Expenditures. N Engl J Med 1999; 340:70-6. - PubMed
-
- Levit K, Cowan C, Braden B, Stiller J, Sensenig A, Lazenby H. National health expenditures in 1997: more slow growth. Health Aff (Millwood) 1998; 17 (6):99-110. - PubMed
-
- Kane NM. Pharmaceutical cost containment and innovation in the United States. Health Pol 1997;41(Suppl):S71-S89. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous