

Imaging findings of cochlear nerve deficiency
- PMID: 11950658
- PMCID: PMC7975095
Imaging findings of cochlear nerve deficiency
Abstract
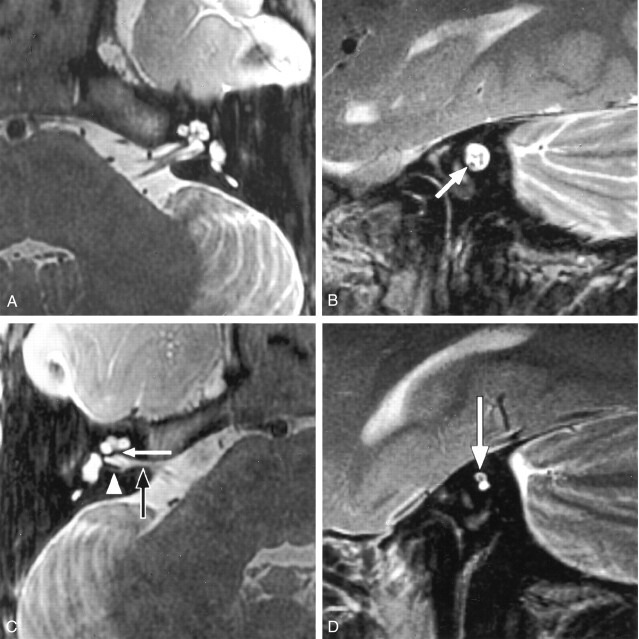
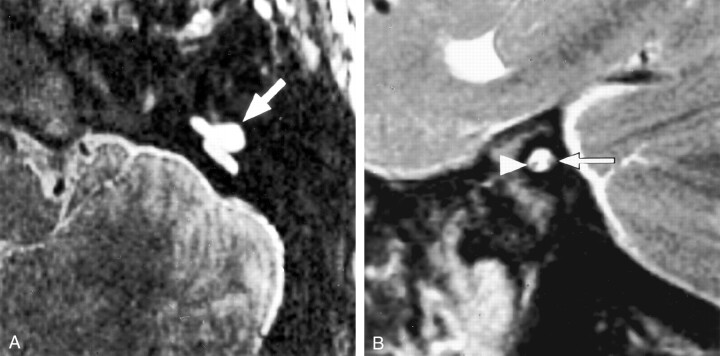
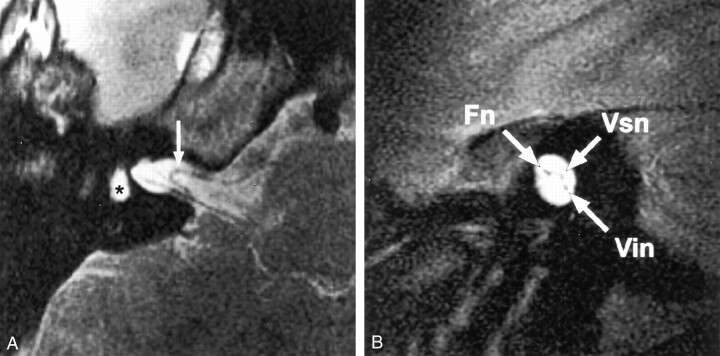
Background and purpose: High-resolution T2-weighted fast spin-echo MR imaging provides excellent depiction of the cisternal and intracanalicular segments of the vestibulocochlear and facial nerves. Absence or reduction in caliber of the cochlear nerve (deficiency) has been described in association with congenital sensorineural hearing loss (SNHL). Depiction of cochlear nerve integrity may be important for diagnosis and management of SNHL.
Methods: We retrospectively reviewed high-resolution T2-weighted fast spin-echo MR images of 22 patients examined for SNHL who had deficiency of the cochlear nerve. Images were evaluated for the presence and comparative size of the component nerves (facial, cochlear, superior vestibular, and inferior vestibular nerves), relative size of the internal auditory canal (IAC), and any associated inner ear abnormalities. The clinical history, results of the clinical examination, and audiometric findings were reviewed for each patient.
Results: Deficiency of the cochlear nerve was observed in 12 patients with congenital SNHL and in 10 patients with acquired SNHL. Hypoplasia of the IAC was observed in association with congenital deficiency of the cochlear nerve in 11 of 12 patients. Deficiency of the cochlear nerve was observed in association with acoustic schwannoma in two cases and with acquired labyrinthine abnormalities in seven cases. Hypoplasia of the IAC was not observed in association with acquired SNHL.
Conclusion: Deficiency of the cochlear nerve can be shown by high-resolution T2-weighted fast spin-echo MR imaging. Deficiency may be observed in association with congenital or acquired SNHL and may be important in the assessment of patients for cochlear implantation. Hypoplasia of the IAC is an indicator of congenital cochlear nerve deficiency.
Figures



References
-
- Casselman JW, Offeciers FE, Govaerts PJ, et al. Aplasia and hypoplasia of the vestibulocochlear nerve: diagnosis with MR imaging. Radiology 1997;202:773–781 - PubMed
-
- Nadol JB Jr, Xu WZ. Diameter of the cochlear nerve in deaf humans: implications for cochlear implantation. Ann Otol Rhinol Laryngol 1992;101:988–993 - PubMed
-
- Felix H, Hoffmann V. Light and electron microscopic investigation of cochlear nerve specimens from profoundly deaf patients. Acta Otolaryngol Suppl 1985;423:67–72 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical