

Review
doi: 10.1136/gut.50.5.733.
Ablative therapy for liver tumours
Affiliations
- PMID: 11950826
- PMCID: PMC1773197
- DOI: 10.1136/gut.50.5.733
Item in Clipboard
Review
Ablative therapy for liver tumours
Gut.
2002 May.
Abstract
Established ablative therapies for the treatment of primary and secondary liver tumours, including percutaneous ethanol injection, cryotherapy, and radiofrequency ablation, are discussed. Newer techniques such as magnetic resonance imaging guided laser interstitial thermal therapy of liver tumours has produced a median survival rate of 40.8 months after treatment. The merits of this newly emerging technique are discussed, together with future developments, such as focused ultrasound therapy, which holds the promise of non-invasive thermoablation treatment on an outpatient basis.
Figures

Vertically orientated double magnet configuration (0.5 T) with a 56 cm gap for the operator to gain access to the patient. A liquid crystal monitor within the bore displays the current magnetic resonance image to the operator.

(Top left to bottom right) Near real time colour thermal map acquired during laser interstitial thermal therapy of colorectal carcinoma metastasis. Images are acquired in the sagittal plane and regularly updated as necrosis develops. The colour scale ranges from blue to green to yellow to red. Once a persistent green colour develops, irreversible necrosis has occurred.
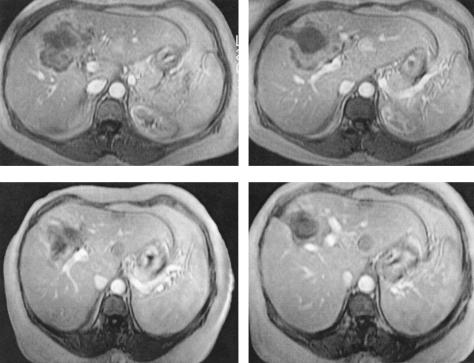
Axial T1 weighted gadolinium enhanced magnetic resonance imaging of the liver in a patient with colorectal carcinoma metastasis four weeks after (top row) the first thermal ablation and four weeks after (bottom row) a second thermal ablation. After the first ablation, low signal non-enhancement in the centre of the metastasis represents necrosis but some enhancing tumour remains around the periphery. After the second ablation no enhancement is seen, and there is uniform low signal representing complete necrosis of the metastasis.
References
-
- OPCS. Office of Population Censuses and Surveys Mortality Statistics. London: HMSO, 1990.
-
- Greenway B. Hepatic metastases from colorectal cancer: resection or not. Br J Surg 1988;75:513–9. - PubMed
-
- Grasso A, Watkinson AF, Tibballs JM, et al. Radiofrequency ablation in the treatment of hepatocellular carcinoma—a clinical viewpoint. J Hepatol 2000;33:667–72. - PubMed
-
- de Jode MG, Lamb GM, Thomas HC, et al. MRI guidance of infra-red laser liver tumour ablations, utilising an open MRI configuration system: technique and early progress. J Hepatol 1999;31:347–53. - PubMed
-
- Scheele J, Altendorf-Hofmann A, Stangle R, et al. Surgical resection of colorectal liver metastases: Gold standard for solitary and radically resectable lesions (in German). Swiss Surg 1996;(suppl 4):4–17. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical