

Phenobarbitone, neonatal seizures, and video-EEG
- PMID: 11978746
- PMCID: PMC1721395
- DOI: 10.1136/fn.86.3.f165
Phenobarbitone, neonatal seizures, and video-EEG
Abstract
Aims: To evaluate the effectiveness of phenobarbitone as an anticonvulsant in neonates.
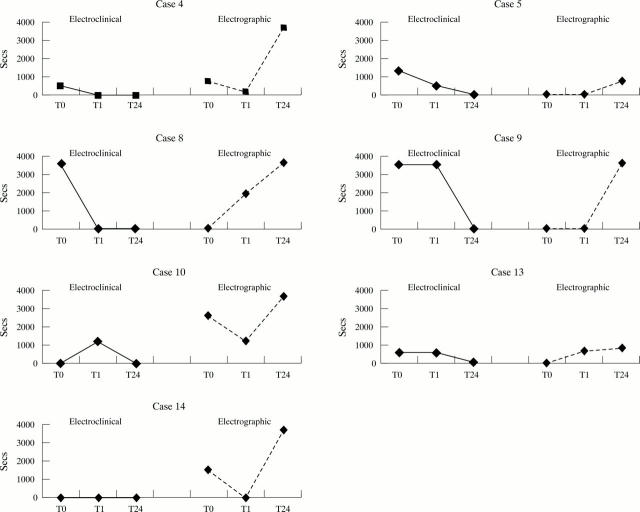
Methods: An observational study using video-EEG telemetry. Video-EEG was obtained before treatment was started, for an hour after treatment was given, two hours after treatment was given, and again between 12 and 24 hours after treatment was given. Patients were recruited from all babies who required phenobarbitone (20-40 mg/kg intravenously over 20 minutes) for suspected clinical seizures and had EEG monitoring one hour before and up to 24 hours after the initial dose. An EEG seizure discharge was defined as a sudden repetitive stereotyped discharge lasting for at least 10 seconds. Neonatal status epilepticus was defined as continuous seizure activity for at least 30 minutes. Seizures were categorised as EEG seizure discharges only (electrographic), or as EEG seizure discharges with accompanying clinical manifestations (electroclinical). Surviving babies were assessed at one year using the Griffiths neurodevelopmental score.
Results: Fourteen babies were studied. Four responded to phenobarbitone; these had normal or moderately abnormal EEG background abnormalities and outcome was good. In the other 10 babies electrographic seizures increased after treatment, whereas electroclinical seizures reduced. Three babies were treated with second line anticonvulsants, of whom two responded. One of these had a normal neurodevelopmental score at one year, but the outcome for the remainder of the whole group was poor.
Conclusion: Phenobarbitone is often ineffective as a first line anticonvulsant in neonates with seizures in whom the background EEG is significantly abnormal.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical