

Magnetic resonance imaging of the infant brain: anatomical characteristics and clinical significance of punctate lesions
- PMID: 11978747
- PMCID: PMC1721406
- DOI: 10.1136/fn.86.3.f171
Magnetic resonance imaging of the infant brain: anatomical characteristics and clinical significance of punctate lesions
Abstract
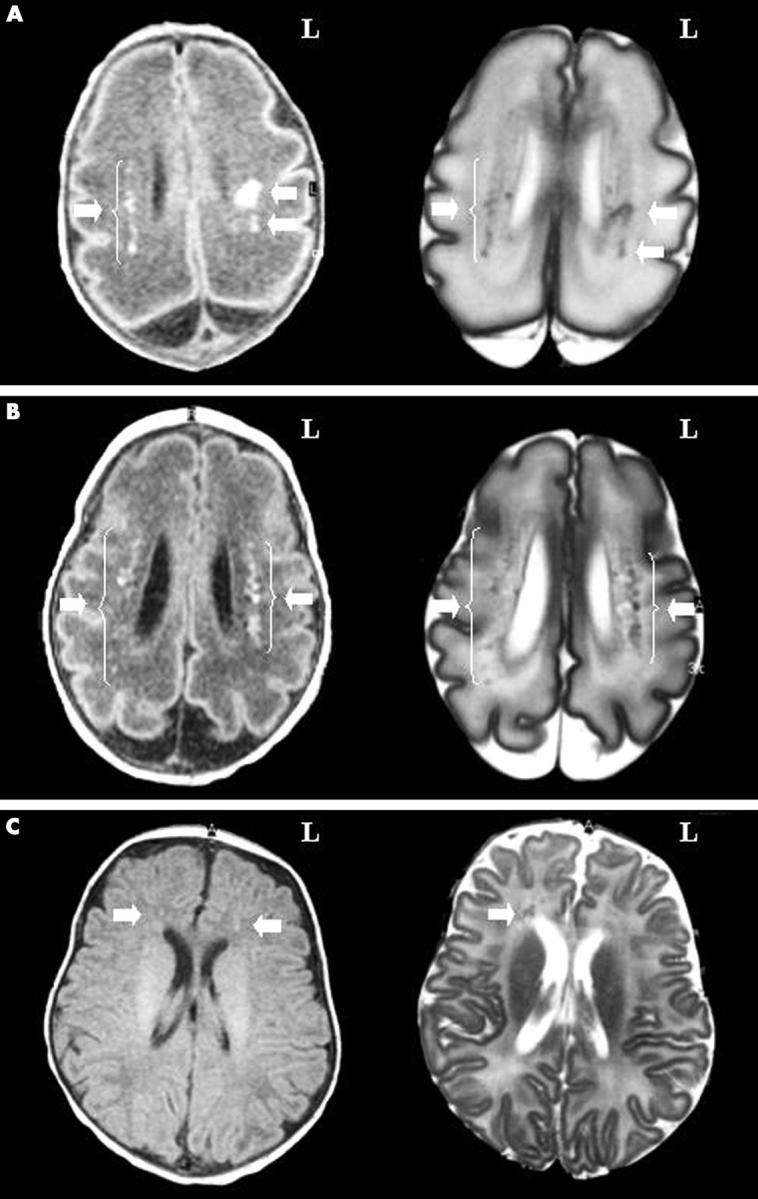
Objective: To describe the magnetic resonance imaging (MRI) characteristics of punctate brain lesions in neonates (number, appearance, distribution, and association with other brain abnormalities) and to relate them to neurodevelopmental outcome.
Methods: A retrospective analysis was performed of 110 MRI brain scans from 92 infants admitted in 1998 to the neonatal intensive care unit. Results of routine neurodevelopmental follow up (1998-2001) in those infants with punctate brain lesions were analysed.
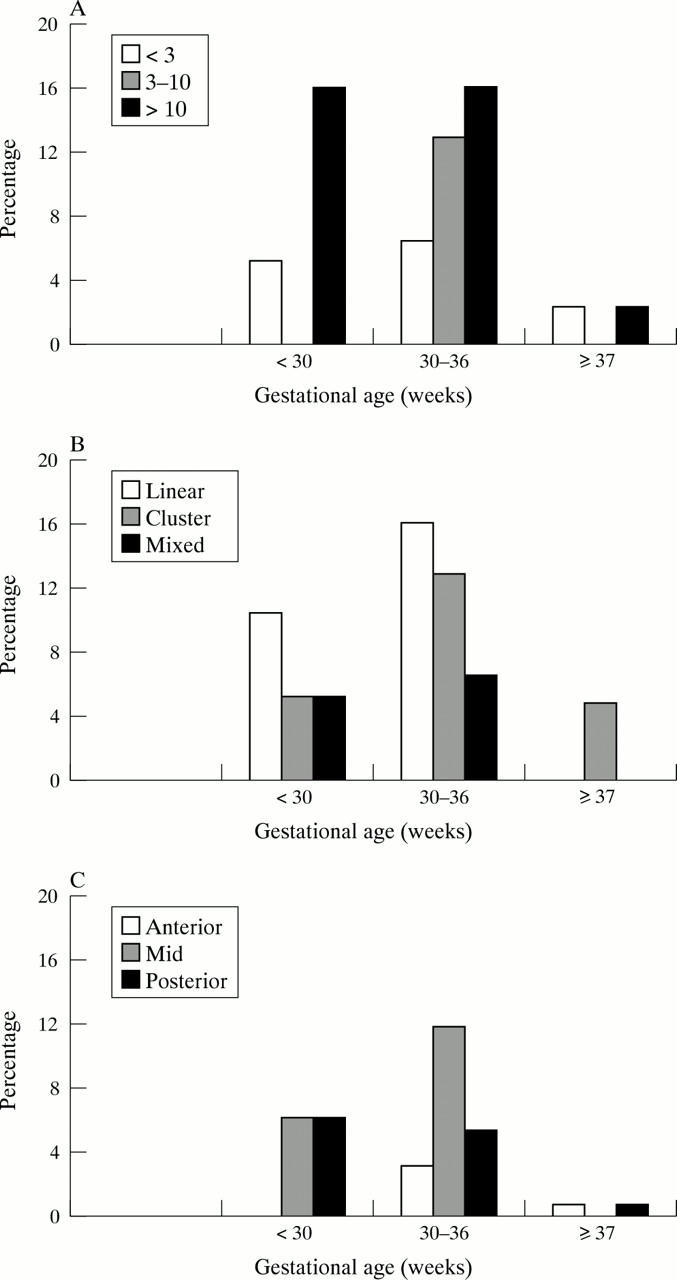
Results: Punctate lesions were observed in 15/50 preterm and 2/42 term infants. In the preterm group, the number of lesions was < 3 in 20%, 3-10 in 27%, and > 10 in 53%. In 14/15 the lesions were linearly organised and located in the centrum semiovale. Other brain abnormalities were absent or minor--that is, "isolated" punctate lesions--in 8/15 and major in 7/15. In the term group, punctate lesions were organised in clusters and no other brain abnormalities were observed. Isolated punctate lesions were observed in 10/17 infants, and a normal neurodevelopmental outcome was seen in 9/10 (mean follow up 29.5 months). One infant showed a slight delay in language development. In the infants with associated brain lesions (7/17, mean follow up 27.5 months), outcome was normal in only two subjects.
Conclusions: Punctate lesions are predominantly seen in preterm infants, are usually linearly organised, and border the lateral ventricles. Isolated punctate lesions may imply a good prognosis, because most of these subjects have a normal neurodevelopmental outcome so far.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical